Results
During the study period, 11,710 endoscopic procedures (5,075 colonoscopies, 627 flexible sigmoidoscopies, 4,450 esophagogastroduodenoscopies, 117 double balloon enteroscopy, 470 endoscopic retrograde cholangiopancreatographies, 761 endoscopic ultrasounds, and 210 percutaneous endoscopic gastrostomy) were performed on 9,683 patients. Patient calls were made by three full-time study personnel. They made at least one telephone call to 1,999 patients (20.6% of all patients in the study period), and ultimately made contact with 1,690 patients (84.5% of those who were called). Of the 1,999 patients called, 1,131 (56.6%) were called once, 530 (26.5%) were called twice, and 338 (16.9%) were called 3 times, for a total of 3,205 calls. For the intention-to-treat analysis, we used 9,683 as the denominator, because our intention was to reach all 9,683 patients. For the per-protocol analysis, we used 1,999 as the denominator, representing the number of patients called 1 or more times.
Twenty-eight true adverse events were identified through the telephone contact method. By using the ASGE grading system (Table 1), 22 (78.5%) were graded as mild, 5 (17.8%) as moderate, and 1 (3.5%) as severe. By comparison, our adverse event tracking MDI identified 93 adverse events. Of these, 43 (46.2%) were mild (P = .003), 34 (36.5%) were moderate (P = .07), 12 (12.9%) were severe (P = .29), and 4 (4.3%) were fatal (P = .57) (Table 3).Telephone query identified pain in 16 patients (57%), bleeding in 6 (21.4%), cardiovascular events in 2 (7.1%), infection in 1 (3.5%), pulmonary in 1 (3.5%), and instrumental (perforation) in 1 (3.5%) (based on the ASGE classification system) (Table 2: www.cghjournal.org/article/S1542-3565(14)01390-1/fulltext). By comparison, MDI event tracking identified pain in 19 (20.4%; P = .0006), bleeding in 16 (17.2%; P = .5871), cardiovascular events in 17 (18.2%; P = .237), instrumental in 16 (17.2%; P = .117), pancreatitis in 6 (6.5%; P = .33), pulmonary in 6 (6.5%; P = 1.00), infection in 4 (4.3%; P = 1.00), integument in 3 (3.2%; P = 1.00), and other in 4 (4.3%; P = .5723).
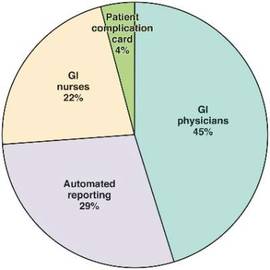
Sources of adverse event reporting with the MDI.
Only 7 events were detected by both methods; the direct patient contact method detected 21 unique cases and the MDI detected 86 unique cases. Together, the two methods identified 107 (1.1%) adverse events over the study period.
The MDI event tracking method had many avenues for reporting adverse events. Of those reported, 73 (78%) were reported by one source, 17 (18.3%) were reported by two sources, and 3 (3.2%) were reported by three or more sources. Of the 73 events that were reported by a single source, 45.2% were reported by physicians within our practice, 28.7% were reported by our automated reporting system, 21.9% were reported by gastroenterology nursing, and 4.2% were reported by patients returning their endoscopic complication cards (Figure 2).
When using the intention-to-treat analysis we found a significantly higher capture rate for adverse events in the MDI method vs. the telephone contact method (P = .0001). The statistical power for the intention-to-treat analysis was 100%. When using the per-protocol analysis, we found no significant difference (P = .099) between the two methods. The statistical power for the per-protocol analysis was 80.7%.
Discussion
Our gastroenterology professional societies have recommended that adverse events associated with endoscopic procedures be identified and tracked to ensure quality and safety in an endoscopic practice2,3,16,17,18 and to identify trends in a practice or provider that might require intervention or improvement.
Tracking adverse events is no easy task. In the past, there has been an assumption that the best way to identify adverse events is by direct patient contact either by telephone, follow-up visits, or mailings.8,10,11,12,19
All of these methods are time and cost intensive. It is our impression that few practices have developed formal programs for tracking adverse events, likely because of these barriers.
This study showed that a multidisciplinary infrastructure to track endoscopic adverse events in a high-volume endoscopy center performs at least as well as a program designed to contact patients directly via telephone, using both intention-to-treat and per-protocol analyses. Furthermore, there was a trend toward capturing more severe adverse events (including fatalities) with the MDI vs. the direct patient contact method.
The costs associated with our internal infrastructure include the cost of the endoscopic complication cards (approximately $1,000 for the study period) and the personnel to enter adverse events into a database. It typically takes 4 hours a week (or 10% of their time) to accomplish this task for a unit that performs approximately 750 endoscopic procedures a week. We acknowledge that this infrastructure does use some resources and is not no-cost. However, many experts agree that quality improvement and reporting processes require dedicated resources that should be considered part of the cost of practice.1
