The Veterans Affairs Patient Safety Center of Inquiry—Suicide Prevention Collaborative: Creating Novel Approaches to Suicide Prevention Among Veterans Receiving Community Services
Bryann DeBeer is the Director of the VA Patient Safety Center of Inquiry – Suicide Prevention Collaborative and a Clinical Research Psychologist; Claire Hoffmire is an Epidemiologist and Health Science Specialist; Nathaniel Mohatt is a Research Psychologist; Germaine Franciosi is a Quality Management Specialist; Edgar Villarreal is a Clinical Psychologist and Program Manager for Suicide Prevention; all at the VA Eastern Colorado Health Care System (VAECHCS). Lindsey Monteith is a Clinical Research Psychologist; Dawn Pierson is a Program Specialist; and Samantha Synett is Suicide Prevention Coordinator; all at the Rocky Mountain Mental Illness, Research, Education and Clinical Center (MIRECC) for Suicide Prevention, Rocky Mountain Regional Veterans Administration Medical Center in Aurora, Colorado. Bryann DeBeer is a Visiting Associate Professor; Claire Hoffmire is an Assistant Professor; and Nathaniel Mohatt is an Assistant Professor in the Department of Physical Medicine and Rehabilitation; Lindsey Monteith is an Associate Professor in the Department of Psychiatry; all at the University of Colorado Anschutz Medical Campus in Aurora, Colorado. Joseph Mignogna is a Clinical Research Psychologist; and Justin Benzer is the Implementation Core Chief; both at the VA VISN 17 Center of Excellence for Research on Returning War Veterans in Waco and the Central Texas Veterans Health Care System. Sylvia Baack is the Director of Quality, Safety, and Value; Kathryn Bongiovanni and Kattina Bryant are Suicide Prevention Coordinators; Stephanie Clafferty and Kimberly Weinberg are Social Work Supervisors; Marjory Williams is the Associate Chief Nurse, Research; all at the Central Texas Veterans Health Care System in Waco, Temple, and Austin. Elisa Borah is the Director of the Institute for Military and Veteran Family Wellness and a Research Associate Professor at the Steve Hicks School of Social Work at the University of Texas at Austin. Craig Bryan is the Stress, Trauma, and Resilience (STAR) Professor at The Ohio State University Wexner Medical Center in Columbus. Ruth Cassidy is the Navy Suicide Prevention Program Manager/Lead Analyst in the 21st Century Sailor Office, Compliance and Competencies Branch in the US Navy, Millington, Tennessee. Jenna Heise is Texas State Suicide Prevention Coordinator in theOffice of Mental Health Coordination, Suicide Prevention Team, Health and Human Services Commission in Austin and Zero Suicide Faculty at Zero Suicide Institute, Education Development Center in Waltham, Massachusetts. Robin Keene is not affiliated with an organization. Joseph Mignogna is an Adjunct Assistant Professor in the Department of Psychiatry and Behavioral Sciences at the College of Medicine, in Temple, Texas. Alan Peterson is a Professor in the Department of Psychiatry and Behavioral Sciences, University of Texas Health Science Center at San Antonio; a Research Health Scientist in the Research and Development Service, South Texas Veterans Health Care System; and a Professor in the Department of Psychology, University of Texas at San Antonio. Nathaniel Mohatt is a Clinical Instructor in the Division of Prevention and Community Research, Department of Psychiatry, Yale School of Medicine. Justin Benzer is an Associate Professor in the Department of Psychiatry, Dell Medical School, University of Texas at Austin.
Author disclosures The authors report no actual or potential conflicts of interest with regard to this article. This work was supported by a Patient Safety Center of Inquiry Grant from the Department of Veterans Affairs National Center for Patient Safety.
Disclaimer The opinions expressed herein are those of the authors and do not necessarily reflect those of Federal Practitioner, Frontline Medical Communications Inc., the US Government, any of its agencies, or any other affiliates
The second PSCI-SPC objective is to develop a toolkit for the implementation of best practices within a VHA-community suicide prevention learning collaborative.Lessons from the development of a successful suicide prevention learning collaborative will be shared through an online guide that other VHA facilities can use to support similar collaborative efforts within their communities. The toolkit will be disseminated across the VHA to assist suicide prevention coordinators and other staff in developing a suicide prevention learning collaborative at their facilities.
PSCI-SPC uses the Zero Suicide framework and the VA/US Department of Defense (DoD) Clinical Practice Guideline for the Assessment and Management of Patients at Risk for Suicide as models for preventing suicide in veterans not enrolled in VHA care.11,32 This implementation toolkit focuses on how to implement suicide prevention best practices into organizations that serve veterans. This toolkit differs from clinical practice guidelines in that it focuses on implementation strategies to promote success and effectively address challenges.
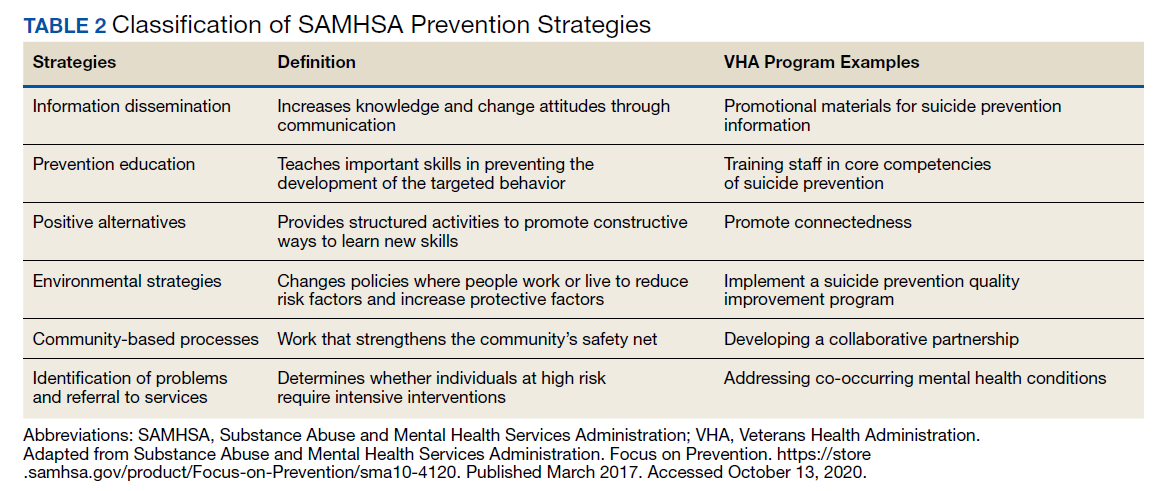
In order to provide a menu of available options for the learning collaborative and resulting toolkit, PSCI-SPC uses a logic model to compare the components of the VHA suicide prevention program, as well as other similar veteran and military suicide prevention programs.7,12,14,21,33,34 These programs are categorized into 2 types of prevention frameworks, the USI model as described above, and the SAMHSA Strategic Prevention Framework (Table 2).35 The SAMHSA framework was designed to promote mental health and prevent substance abuse, yet the derived classification is also applicable to suicide prevention programs.35 The results of the logic model comparison form the basis of the best practice interventions for the learning collaborative and initial toolkit. In addition to the best practice interventions, the toolkit consists of documents describing how to develop a veteran suicide prevention learning collaborative, as well as tools for learning collaborative members. Current tool development includes workbooks to guide collaborative members through the implementation process, guides for community organizations in implementing suicide prevention screening and risk assessment, a standard operating procedure for suicide prevention in a veterans court, and peer support training for veteran suicide prevention.
The methods to achieve Objective 2 include regular discussions with the VHA-learning collaborative on current best practices, identifying gaps and overlap of community programs. Successes and challenges of implementing suicide prevention best practices into learning collaborative organizations will be documented and incorporated into the toolkit. The learning collaborative will work iteratively as a team to improve the toolkit. Once complete, the toolkit will be disseminated to other VHA health care systems nationally, as well as to other state or regional partners that the learning collaborative identifies. A plan is under development for national suicide prevention entities to also disseminate the toolkit to lessen the burden of veteran suicide through their stakeholder base.
Objective 3: High-Risk Veterans Not Receiving VHA Care
Although veterans not receiving VHA care account for a number of veteran deaths by suicide, we are not aware of any current VHA programs that provide temporary psychotherapy and intensive case management to at-risk veterans ineligible for VHA care who are in need of immediate care while an appropriate permanent community placement is identified. In the current system, veterans in the community can present to VHA suicide prevention services through several different systems, including referrals to VHA and the Veterans Crisis Line (VCL). However, a portion of VCL calls are from veterans whose VHA eligibility is unknown or who are ineligible for services. If veterans are at imminent risk for suicide, emergency care is coordinated for them. However, if veterans are not at imminent suicide risk they are referred to the local suicide prevention coordinator and instructed to independently work toward determining their VHA eligibility.