The Veterans Affairs Patient Safety Center of Inquiry—Suicide Prevention Collaborative: Creating Novel Approaches to Suicide Prevention Among Veterans Receiving Community Services
Bryann DeBeer is the Director of the VA Patient Safety Center of Inquiry – Suicide Prevention Collaborative and a Clinical Research Psychologist; Claire Hoffmire is an Epidemiologist and Health Science Specialist; Nathaniel Mohatt is a Research Psychologist; Germaine Franciosi is a Quality Management Specialist; Edgar Villarreal is a Clinical Psychologist and Program Manager for Suicide Prevention; all at the VA Eastern Colorado Health Care System (VAECHCS). Lindsey Monteith is a Clinical Research Psychologist; Dawn Pierson is a Program Specialist; and Samantha Synett is Suicide Prevention Coordinator; all at the Rocky Mountain Mental Illness, Research, Education and Clinical Center (MIRECC) for Suicide Prevention, Rocky Mountain Regional Veterans Administration Medical Center in Aurora, Colorado. Bryann DeBeer is a Visiting Associate Professor; Claire Hoffmire is an Assistant Professor; and Nathaniel Mohatt is an Assistant Professor in the Department of Physical Medicine and Rehabilitation; Lindsey Monteith is an Associate Professor in the Department of Psychiatry; all at the University of Colorado Anschutz Medical Campus in Aurora, Colorado. Joseph Mignogna is a Clinical Research Psychologist; and Justin Benzer is the Implementation Core Chief; both at the VA VISN 17 Center of Excellence for Research on Returning War Veterans in Waco and the Central Texas Veterans Health Care System. Sylvia Baack is the Director of Quality, Safety, and Value; Kathryn Bongiovanni and Kattina Bryant are Suicide Prevention Coordinators; Stephanie Clafferty and Kimberly Weinberg are Social Work Supervisors; Marjory Williams is the Associate Chief Nurse, Research; all at the Central Texas Veterans Health Care System in Waco, Temple, and Austin. Elisa Borah is the Director of the Institute for Military and Veteran Family Wellness and a Research Associate Professor at the Steve Hicks School of Social Work at the University of Texas at Austin. Craig Bryan is the Stress, Trauma, and Resilience (STAR) Professor at The Ohio State University Wexner Medical Center in Columbus. Ruth Cassidy is the Navy Suicide Prevention Program Manager/Lead Analyst in the 21st Century Sailor Office, Compliance and Competencies Branch in the US Navy, Millington, Tennessee. Jenna Heise is Texas State Suicide Prevention Coordinator in theOffice of Mental Health Coordination, Suicide Prevention Team, Health and Human Services Commission in Austin and Zero Suicide Faculty at Zero Suicide Institute, Education Development Center in Waltham, Massachusetts. Robin Keene is not affiliated with an organization. Joseph Mignogna is an Adjunct Assistant Professor in the Department of Psychiatry and Behavioral Sciences at the College of Medicine, in Temple, Texas. Alan Peterson is a Professor in the Department of Psychiatry and Behavioral Sciences, University of Texas Health Science Center at San Antonio; a Research Health Scientist in the Research and Development Service, South Texas Veterans Health Care System; and a Professor in the Department of Psychology, University of Texas at San Antonio. Nathaniel Mohatt is a Clinical Instructor in the Division of Prevention and Community Research, Department of Psychiatry, Yale School of Medicine. Justin Benzer is an Associate Professor in the Department of Psychiatry, Dell Medical School, University of Texas at Austin.
Author disclosures The authors report no actual or potential conflicts of interest with regard to this article. This work was supported by a Patient Safety Center of Inquiry Grant from the Department of Veterans Affairs National Center for Patient Safety.
Disclaimer The opinions expressed herein are those of the authors and do not necessarily reflect those of Federal Practitioner, Frontline Medical Communications Inc., the US Government, any of its agencies, or any other affiliates
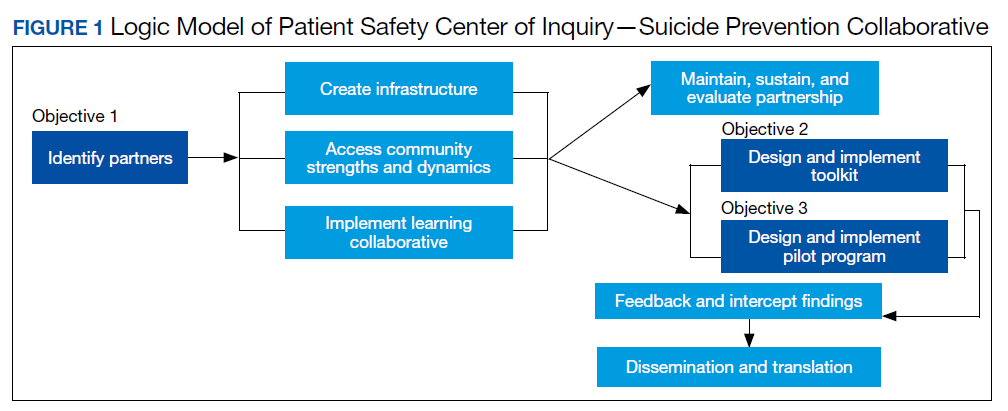
VHA Patient Safety Center of Inquiry-Suicide Prevention Collaborative (PSCI-SPC), funded by the VHA National Center for Patient Safety, aims to help fill the gap in community-based suicide prevention for veterans. PSCI-SPC is located within the VHA Rocky Mountain Mental Illness Research, Education, and Clinical Center in Aurora, Colorado. The overarching mission of PSCI-SPC is to develop, implement, and evaluate practical solutions to reduce suicide among veterans not receiving VHA care. PSCI-SPC serves as a national clinical innovation and dissemination center for best practices in suicide prevention for organizations that serve veterans who receive care in the community. PSCI-SPC creates products to support dissemination of these practices to other VAMCs and works to ensure these programs are sustainable. PSCI-SPC focuses on 3 primary objectives. All PSCI-SPC projects are currently underway.
Objective 1: Growing a Community Learning Collaborative
Acknowledging that nearly two-thirds of veterans who die by suicide do not use VHA services, PSCI-SPC aims to reduce suicide among all veterans by expanding the reach of best practices for suicide prevention to veterans who receive myriad services in the community.27 Community organizations are defined here as organizations that may in some way serve, interact with, or work with veterans, and/or employ veterans. Examples include non-VHA health care systems, public services such as police and fire departments, nonprofit organizations, mental health clinics, and veterans’ courts. As veterans increasingly seek health care and other services within their communities, the success of suicide prevention will be influenced by the capability of non-VHA public and private organizations. Objective 1, therefore, seeks to develop a VHA-community collaborative that can be leveraged to improve systems of suicide prevention.
Current programs in the VHA have focused on implementation of suicide prevention awareness and prevention education campaigns instead of grassroots partnerships that are intended to be sustainable. Additionally, these programs typically lack the capacity and systems to sustain numerous meaningful community partnerships. Traditionally, community organizations have been hesitant to partner with government agencies, such as the VHA, due to histories of institutional mistrust and bureaucracy.28
The PSCI-SPC model for developing a VHA-community collaborative partnership draws from the tradition of community-based participatory research. The best community-based participatory research practices are to build on strengths and resources within the local community; develop collaborative, equitable partnerships that involve an empowering and power-sharing process; foster colearning, heuristics, and capacity building among partners; and focus on systems development using an iterative process. These practices also are consistent with the literature on learning collaboratives.29-31
The premise for a learning collaborative is to bridge the gap between knowledge and practice in health care.31 Figure 1 depicts how this collaborative was developed, and how it supports Objectives 2 and 3. To achieve Objective 1, we developed a VHA-learning collaborative of 13 influential community partners in the Denver and Colorado Springs region of Colorado. The VHA team consists of a learning collaborative leader, a program manager, and a program support assistant. The principal investigator attends and contributes to all meetings. Learning collaborative partners include a university psychology clinic that focuses on veterans’ care, 3 veterans service organizations, a mental health private practice, a university school of nursing, a community mental health center, veterans’ courts, and 5 city departments.
These partners participated in qualitative interviews to identify where gaps and breakdowns were occurring. With this information, the PSCI-SPC team and VHA-learning collaborative held a kickoff event. At this meeting the team discussed the qualitative findings, provided veteran suicide prevention information, and basic information regarding suicide prevention program building and implementation science.
Throughout quarterly learning collaborative meetings and monthly facilitation calls, we have worked to develop a blueprint and an action plan for each partner to develop best practices for dissemination to aid in providing consistency in the standard of care. A postimplementation event will be held to identify successes and challenges encountered while operationalizing project action plans.
Currently, activities of the learning collaborative are making a large impact on the community. Not all collaborative members track information regarding their populations served, nor specific metrics on veterans encountered. Even so, of those who do capture metrics, suicide prevention program components implemented by the collaborative will impact more than 21,000 individuals and at least 2,500 known veterans. In addition, 52 new connections have been made between community organizations or between community organizations and the VHA, and > 300 individuals have been trained.The learning collaborative support team has assisted in the dissemination of a large resource list for veterans. As the learning collaborative is ongoing and we are working with organizations to improve their data collection and analytics, we expect these numbers to increase. We anticipate that the learning collaborative will develop a stronger suicide prevention safety net within the community. In addition, we expect increased referrals of at-risk veterans to the VHA and enhance the long-term continuity of care between community and VHA services.