The Veterans Affairs Patient Safety Center of Inquiry—Suicide Prevention Collaborative: Creating Novel Approaches to Suicide Prevention Among Veterans Receiving Community Services
Bryann DeBeer is the Director of the VA Patient Safety Center of Inquiry – Suicide Prevention Collaborative and a Clinical Research Psychologist; Claire Hoffmire is an Epidemiologist and Health Science Specialist; Nathaniel Mohatt is a Research Psychologist; Germaine Franciosi is a Quality Management Specialist; Edgar Villarreal is a Clinical Psychologist and Program Manager for Suicide Prevention; all at the VA Eastern Colorado Health Care System (VAECHCS). Lindsey Monteith is a Clinical Research Psychologist; Dawn Pierson is a Program Specialist; and Samantha Synett is Suicide Prevention Coordinator; all at the Rocky Mountain Mental Illness, Research, Education and Clinical Center (MIRECC) for Suicide Prevention, Rocky Mountain Regional Veterans Administration Medical Center in Aurora, Colorado. Bryann DeBeer is a Visiting Associate Professor; Claire Hoffmire is an Assistant Professor; and Nathaniel Mohatt is an Assistant Professor in the Department of Physical Medicine and Rehabilitation; Lindsey Monteith is an Associate Professor in the Department of Psychiatry; all at the University of Colorado Anschutz Medical Campus in Aurora, Colorado. Joseph Mignogna is a Clinical Research Psychologist; and Justin Benzer is the Implementation Core Chief; both at the VA VISN 17 Center of Excellence for Research on Returning War Veterans in Waco and the Central Texas Veterans Health Care System. Sylvia Baack is the Director of Quality, Safety, and Value; Kathryn Bongiovanni and Kattina Bryant are Suicide Prevention Coordinators; Stephanie Clafferty and Kimberly Weinberg are Social Work Supervisors; Marjory Williams is the Associate Chief Nurse, Research; all at the Central Texas Veterans Health Care System in Waco, Temple, and Austin. Elisa Borah is the Director of the Institute for Military and Veteran Family Wellness and a Research Associate Professor at the Steve Hicks School of Social Work at the University of Texas at Austin. Craig Bryan is the Stress, Trauma, and Resilience (STAR) Professor at The Ohio State University Wexner Medical Center in Columbus. Ruth Cassidy is the Navy Suicide Prevention Program Manager/Lead Analyst in the 21st Century Sailor Office, Compliance and Competencies Branch in the US Navy, Millington, Tennessee. Jenna Heise is Texas State Suicide Prevention Coordinator in theOffice of Mental Health Coordination, Suicide Prevention Team, Health and Human Services Commission in Austin and Zero Suicide Faculty at Zero Suicide Institute, Education Development Center in Waltham, Massachusetts. Robin Keene is not affiliated with an organization. Joseph Mignogna is an Adjunct Assistant Professor in the Department of Psychiatry and Behavioral Sciences at the College of Medicine, in Temple, Texas. Alan Peterson is a Professor in the Department of Psychiatry and Behavioral Sciences, University of Texas Health Science Center at San Antonio; a Research Health Scientist in the Research and Development Service, South Texas Veterans Health Care System; and a Professor in the Department of Psychology, University of Texas at San Antonio. Nathaniel Mohatt is a Clinical Instructor in the Division of Prevention and Community Research, Department of Psychiatry, Yale School of Medicine. Justin Benzer is an Associate Professor in the Department of Psychiatry, Dell Medical School, University of Texas at Austin.
Author disclosures The authors report no actual or potential conflicts of interest with regard to this article. This work was supported by a Patient Safety Center of Inquiry Grant from the Department of Veterans Affairs National Center for Patient Safety.
Disclaimer The opinions expressed herein are those of the authors and do not necessarily reflect those of Federal Practitioner, Frontline Medical Communications Inc., the US Government, any of its agencies, or any other affiliates
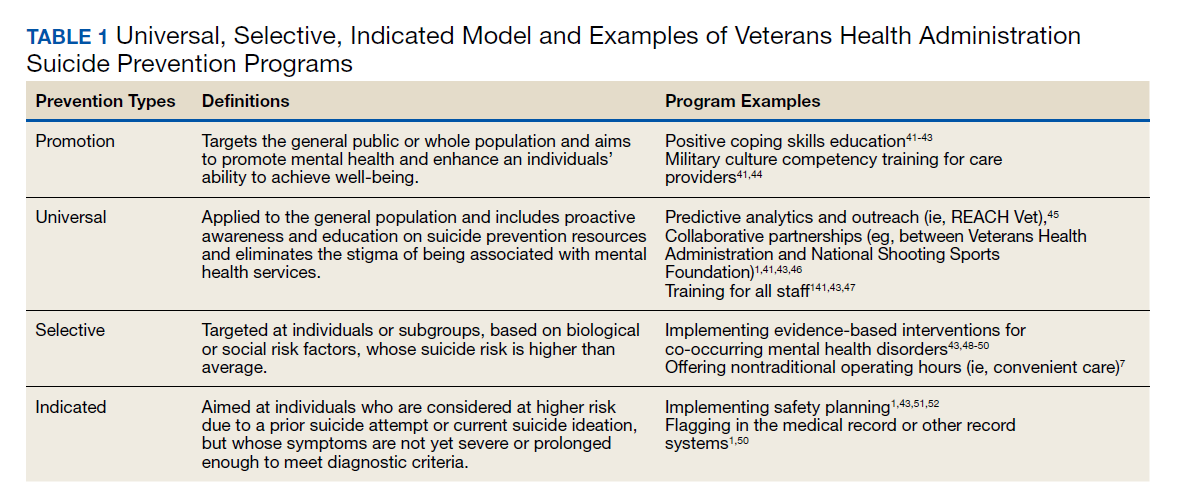
In response to the high rates of veteran suicide deaths, the US Department of Veterans Affairs (VA) has developed a broad, multicomponent suicide prevention program that is unparalleled in private US health care systems.4,7 Suicide prevention efforts are led and implemented by both the VHA National Center for Patient Safety and the VHA Office of Mental Health and Suicide Prevention. Program components are numerous and multifaceted, falling within the broad promotion and prevention strategies outlined by the National Academy of Medicine (NAM).1,8-11 The NAM continuum of prevention model encompassing multiple strategies is also referred to as the Universal, Selective, Indicated (USI) Model.7,8,10 The VHA suicide prevention program contains a wide spread of program components, making it both comprehensive and innovative (Table 1).
Although significant momentum and progress has been made within the VHA, policy set by legislation has historically limited access to VHA health care services to VHA-eligible veterans. This is particularly concerning given the rising suicide rates among veterans not engaged in VHA care.2 Adding to this complexity, recent legislation has increased veterans’ access to non-VHA health care, in addition to their existing access through Medicare, Medicaid, and other health care programs.12-14 Best practices for suicide prevention are not often implemented in the private sector; thus, these systems are ill prepared to adequately meet the suicide prevention care needs of veterans.4,15-18 Furthermore, VHA and non-VHA services generally are not well coordinated, and private sector health care providers (HCPs) are not required to complete a commensurate level of suicide prevention training as are VHA HCPs.16-18 Most non-VHA HCPs do not receive military cultural competence training.19 These issues create a significant gap in suicide prevention services and may contribute to the increases in suicide rates in veterans who do not receive VHA care. Thus, changes in policy to increase access through private sector care may have paradoxical effects on veteran suicide deaths. To impact the veteran suicide rate, VHA must develop and disseminate best practices for veterans who use non-VHA services.
A Roadmap to Suicide Prevention
There is significant momentum at the federal level regarding this issue. The President’sRoadmap to Empower Veterans and End the National Tragedy ofSuicide (Executive Order 13,861) directs the VHA to work closely with community organizations to improve veteran suicide prevention.20 The VHA and partners, such as the Substance Abuse and Mental Health Services Administration (SAMHSA), are bridging this gap with collaborative efforts that increase suicide prevention resources for veterans living in the community through programs such as the Governor’s Challenges to Prevent Suicide Among Service Members, Veterans, and their Families. These programs intend to empower communities to develop statewide, strategic action plans to prevent veteran suicide.7,21-24
In addition to partnerships, VHA has built other aspects of outreach and intervention into its programming. A key VHA initiative is to “know all veterans” by committing to identifying and reaching out to all veterans who may be at risk for suicide.22 The VHA has committed to offering “emergency stabilization care for former service members who present at the facility with an emergent mental health need” regardless of eligibility.25 The intent is to provide temporary emergent mental health care to veterans who are otherwise ineligible for care, such as those who were discharged under other-than-honorable conditions while the VHA determines eligibility status.26 However, veterans must meet certain criteria, and there is a limit on services.
Although services are being expanded to reach veterans who do not access VHA health care, how to best implement these new directives with regard to suicide prevention is unclear. Strategic development and innovations to expand suicide prevention care to veterans outside the current reach of VHA are desperately needed.