Christine Hunt is a Physician Affiliate, Marsha Turner is a Research Health Science Specialist at the Cooperative Studies Program Epidemiology Center, and Rachel Britt is a Hepatology Clinical Pharmacy Specialist, all at Durham Veterans Affairs Health Care System in North Carolina. Elizabeth Gifford is an Assistant Research Professor at the Sanford School of Public Policy at Duke University in Durham. Grace Su is a Professor of Medicine at the VA Ann Arbor Healthcare Systems in Michigan and at the University of Michigan in Ann Arbor. Christine Hunt also is an Adjunct Associate Professor of Medicine at Duke University Medical Center in Durham, North Carolina.
Author disclosures The authors report no actual or potential conflicts of interest with regard to this article.
Disclaimer The opinions expressed herein are those of the authors and do not necessarily reflect those of Federal Practitioner, Frontline Medical Communications Inc., the US Government, or any of its agencies.
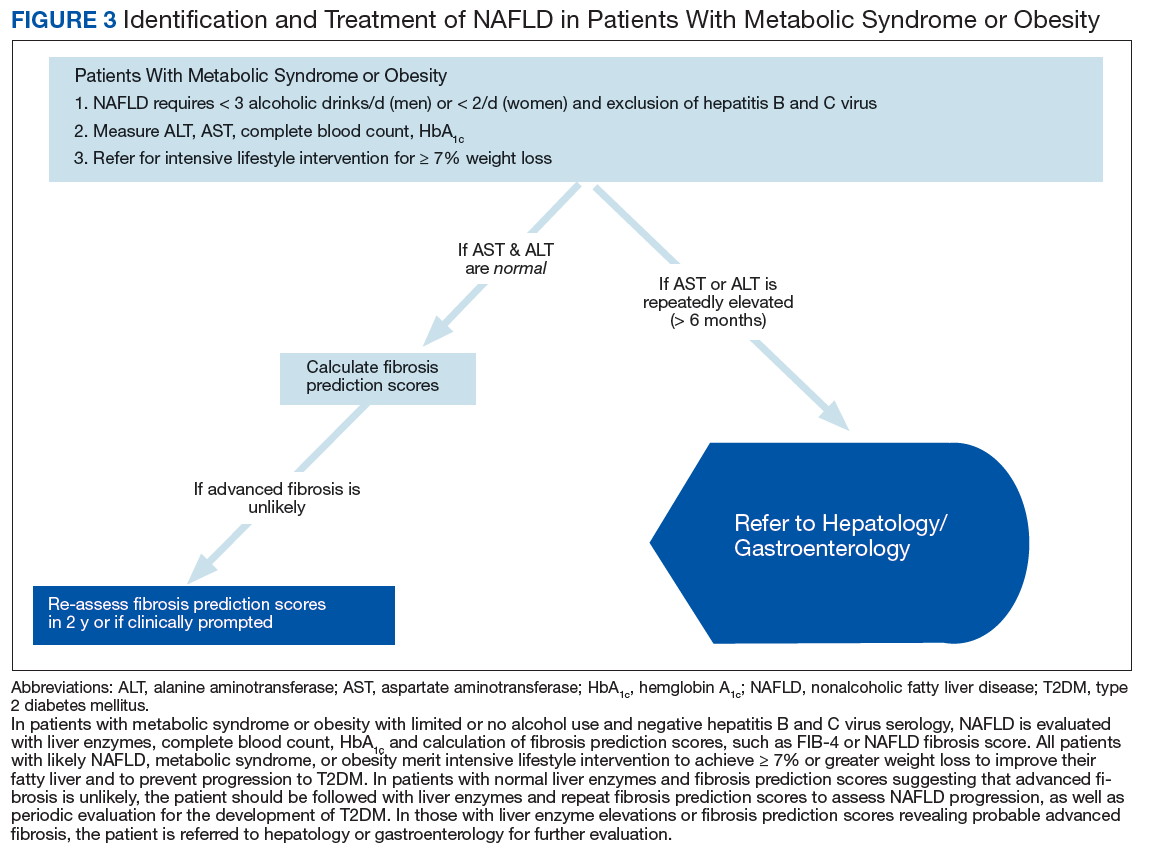
To identify NAFLD, patients with metabolic syndrome and modest or no alcohol use are first assessed for liver injury with ALT, AST, and complete blood count (Figure 3; Case 1).16
Among patients presenting with incidental liver enzyme elevations to primary care, NAFLD was the most common cause.38
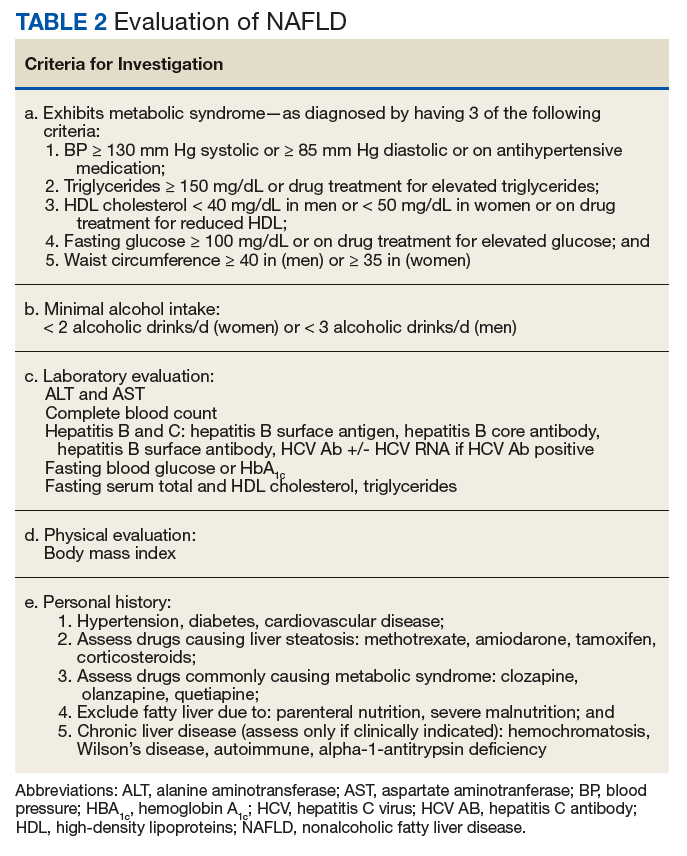
Next, common underlying liver diseases that cause liver injury should be excluded by hepatitis B and C virus serology.11,16 Other underlying liver diseases are uncommon and should be assessed only if clinically indicated.
After excluding secondary causes of fatty liver (eg, drugs causing steatosis, parenteral nutrition, severe malnutrition, etc), NAFLD is likely, particularly in those displaying fatty liver or steatosis on liver imaging (Table 2).11,16
Evaluation of fasting glucose or hemoglobin A1c (HbA1c)can identify undiagnosed T2DM. NAFL, or simple steatosis, is independently associated with an increased risk of T2DM, cardiovascular and kidney disease, yet not overall mortality.16 Over 10 to 20 years, few patients (4%) with simple steatosis progress to cirrhosis.39In contrast, NAFLD advanced fibrosis significantly increases overall and liver-related mortality and can be assessed with high probability by calculating the patient’s FIB-4, even in those with normal liver enzymes.11,16 Patients with highly probable advanced fibrosis merit evaluation by hepatology or gastroenterology (Figure 3).
In NAFLD, simple steatosis can resolve, and NASH can significantly improve with 7% to 10% weight loss.16,23,40 Patients with simple steatosis on imaging and normal liver enzymes should be monitored with periodic liver enzymes and fibrosis prediction scores (eg, FIB-4) and encouraged to pursue intensive lifestyle intervention.16,33 Without weight loss and exercise interventions metabolic syndrome, T2DM, and NAFLD may progress.
Patients with combined liver steatosis and liver enzyme elevations may exhibit NASH and warrant an evaluation by a hepatologist or gastroenterologist for consideration of additional testing or liver biopsy.16While ALT elevations often have been used as a marker of NASH, ALT can be normal in NASH and in advanced fibrosis.41,42 A liver biopsy is required to establish the diagnosis of NASH, which progresses to cirrhosis in 15% to 20% over a 10- to 20-year follow-up period (Case 2).39 Fibrosis prediction scores also can evaluate the probability of advanced fibrosis in these patients.
Encouraging Patients to Pursue Intensive Lifestyle InterventionS
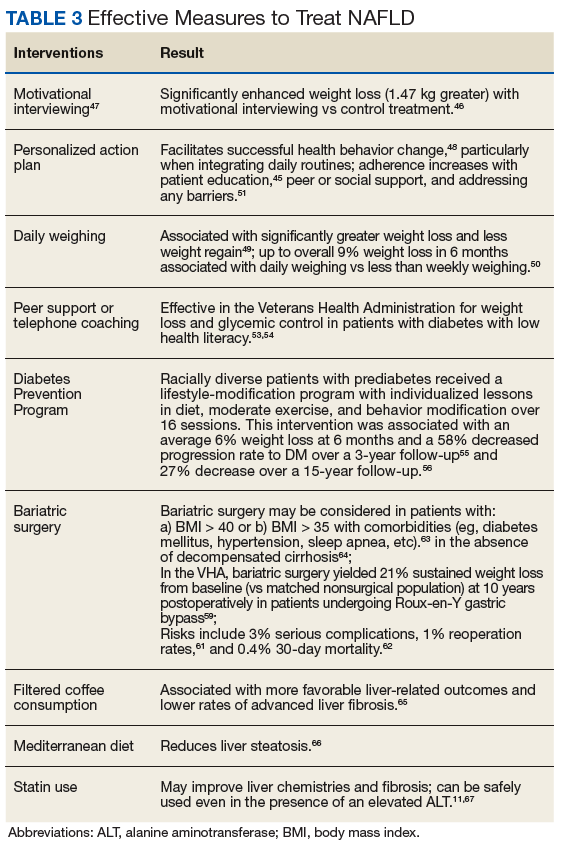
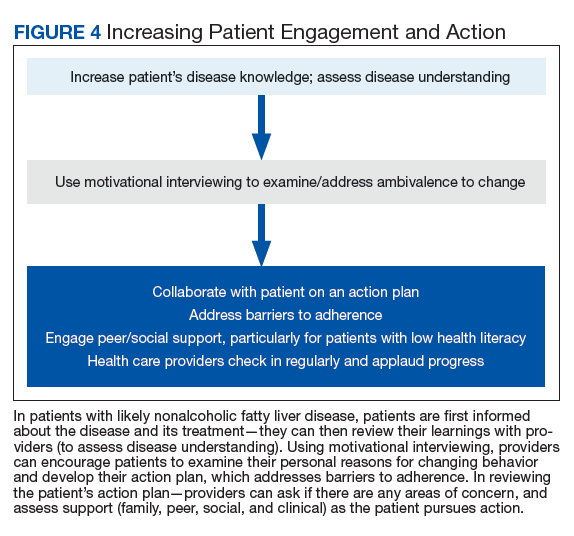
Most veterans wish to collaborate in their care (Table 3, Figure 4) yet experience many barriers, such as low health literacy, high rates of comorbidities, and ongoing drug/alcohol misuse.43,44
To motivate patients to action to prevent the progression of NAFLD, patients must understand how it affects the development of T2DM, cardiovascular disease, and liver disease and the value of the intervention. To enhance disease understanding, the VHA provides a simple 2-page patient information sheet about NAFLD and its treatment.45 A 2-page pictorial patient education handout on NAFLD and its treatment is available as well (eAppendix)
In addition to patient education, motivational interviewing significantly improves weight loss, resulting in a 3.3 lb (1.5 kg) increased weight loss in the intervention group vs the control group in weight loss studies.46By being supportive, empathic, and clearly sharing the rationale for change, motivational interviewing is a collaborative conversation to guide patients to strengthen their motivation and commitment to change.47 It helps patients examine and address their ambivalence—most recognize they should exercise and lose weight, but it can be difficult.
To start the conversation, the health care provider can explain that NAFLD increases the risk of T2DM, heart disease, and liver injury or scarring and can be effectively treated (or improved) with modest weight loss and regular exercise (ie, 14 lb weight loss if 200 lb, or 21 lb weight loss if 300 lb). Exercise can start with a 5-minute walk and build to 30 minutes daily). Then, the provider can ask the following 4 questions: