Christine Hunt is a Physician Affiliate, Marsha Turner is a Research Health Science Specialist at the Cooperative Studies Program Epidemiology Center, and Rachel Britt is a Hepatology Clinical Pharmacy Specialist, all at Durham Veterans Affairs Health Care System in North Carolina. Elizabeth Gifford is an Assistant Research Professor at the Sanford School of Public Policy at Duke University in Durham. Grace Su is a Professor of Medicine at the VA Ann Arbor Healthcare Systems in Michigan and at the University of Michigan in Ann Arbor. Christine Hunt also is an Adjunct Associate Professor of Medicine at Duke University Medical Center in Durham, North Carolina.
Author disclosures The authors report no actual or potential conflicts of interest with regard to this article.
Disclaimer The opinions expressed herein are those of the authors and do not necessarily reflect those of Federal Practitioner, Frontline Medical Communications Inc., the US Government, or any of its agencies.
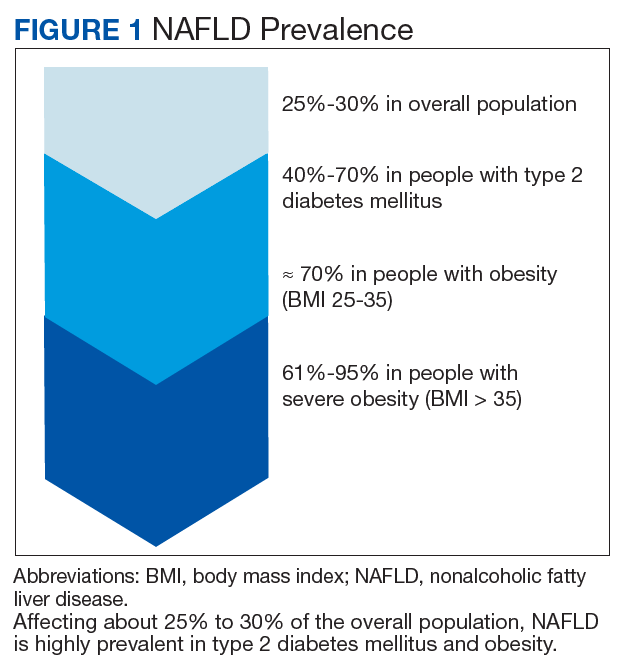
Nonalcoholic fatty liver disease (NAFLD) is a silent epidemic affecting nearly 1 in 3 Americans and is increasing within the Veterans Health Administration (VHA).1,2 NAFLD independently increases the risk of type 2 diabetes mellitus (T2DM), cardiovascular disease, chronic kidney disease, cirrhosis, liver cancer, and death and impairs health-related quality of life (QOL).3 NAFLD primarily affects those with metabolic risk factors (prediabetes, T2DM, and metabolic syndrome) or obesity (Figure 1).4,5
In the US, 1 in 3 adults have prediabetes and 1 in 10 have T2DM (increasing to 1 in 4 aged ≥ 65 years).6 Among veterans, obesity affects 31% within 6 years postdeployment and 41% overall who receive VHA care.7,8 Other patient characteristics associated with higher rates of NAFLD include Hispanic ethnicity and older age.9-11
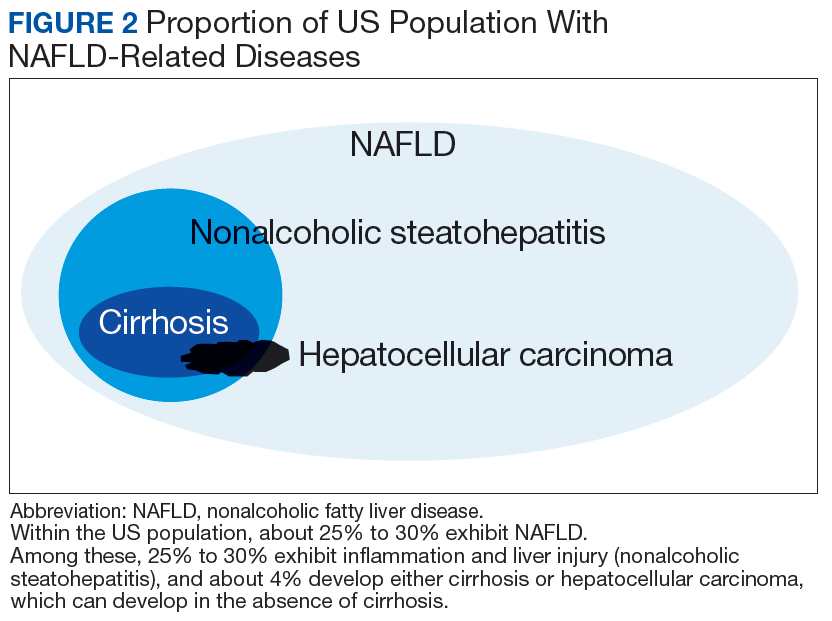
Among those with NAFLD, most have nonalcoholic fatty liver (NAFL), or simple steatosis, affecting > 5% of liver cells (Figure 2).12
However, 25% to 30% exhibit nonalcoholic steatohepatitis (NASH), with steatosis, inflammation, hepatocyte injury, and often alanine aminotransferase (ALT) elevations.13About 4% of patients progress to cirrhosis and/or hepatocellular carcinoma(HCC) on 7- to 15-year follow-up (with 9% cirrhosis or end-stage liver disease rates in 1 recent study with up to 23-year follow-up).1,14
In most patients (80%), NAFLD progresses slowly over decades. The progression is related to continuing insulin resistance.15,16 Greater disease progression is seen in patients with T2DM or concomitant chronic liver disease (such as hepatitis C).10,11,16 Patients with NAFLD who develop advanced fibrosis or cirrhosis experience increased rates of overall mortality, liver-related events, and liver transplantation.1,9,17,18 Within the VHA, NAFLD is the third most common cause of cirrhosis and HCC, occurring at an average age of 66 and 70 years, respectively.19Less commonly, HCC also can occur in NAFLD without cirrhosis.20
Although no pharmaceuticals are yet approved to treat NAFLD, even modest weight loss is beneficial. For example, weight loss > 4% improves fatty liver, ≥ 7% improves liver inflammation, and ≥ 10% decreases liver fibrosis (or scarring).21-23 In patients with a prior lack of success with weight loss, weight loss medications may be beneficial for short-term use.24 When comparing the effects of diet, exercise, obesity pharmacotherapy, and combinations for these approaches, intensive lifestyle modification with exercise had the greatest, most enduring benefit.25 Additionally, bariatric (weight loss) surgery has significantly improved health and liver-related outcomes for patients with NASH.26
In at-risk veterans, NAFLD has myriad negative effects on health and QOL. To improve its early identification and management in the VHA, we summarize strategies that all providers can use to screen and treat patients for this condition.
Screening for Advanced Fibrosis
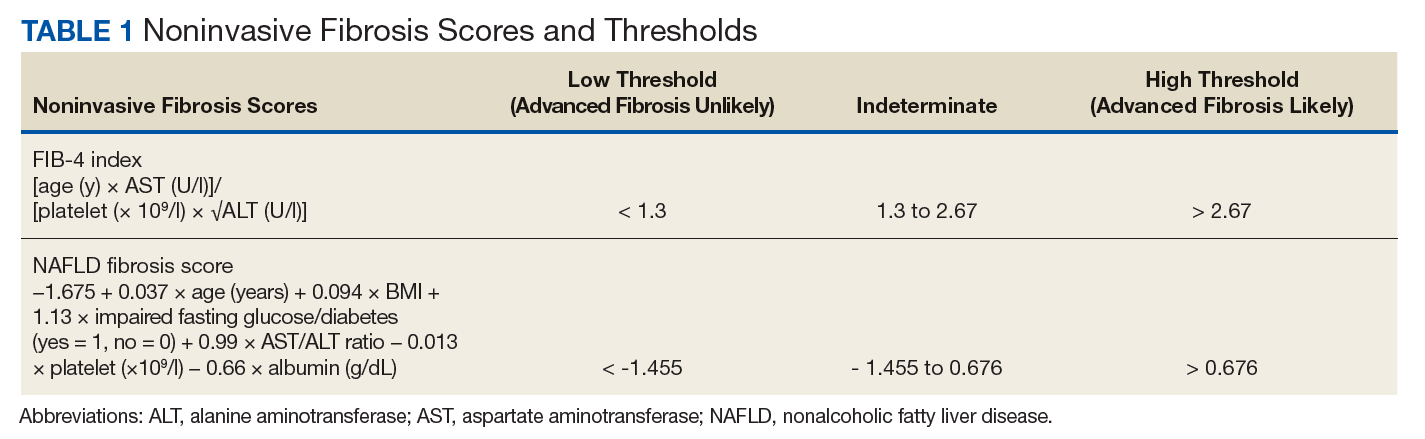
Advanced fibrosis in NAFLD is diagnosed by analyzing adequately sized liver biopsies.27,28 However, noninvasive approaches to quantify advanced fibrosis by imaging or use of a simple fibrosis prediction score also are available. Imaging modalities include measuring liver stiffness, using transient elastography (FibroScan, Waltham, MA) or magnetic resonance elastography.1,29-31 Fibrosis prediction scores use common clinical and laboratory data to predict the presence or absence of advanced fibrosis (Table 1).29
Of these, the fibrosis-4 (FIB-4) index requires only ALT, aspartate aminotransferase (AST), platelet count, and age to calculate the score and performs similarly to the NAFLD fibrosis score.32-35 FIB-4 and the NAFLD fibrosis score are validated in ethnically diverse populations, recommended in evidence-based guidelines, and can be calculated using online calculators (eg, FIB-4).11,16,33 The easily summed BARD score also detects NAFLD advanced fibrosis yet incorrectly identified advanced fibrosis in many patients without liver biopsy evidence of advanced fibrosis in a recent VHA study.36,37 With increasing VHA rates of NAFLD, these scores are a simple way to identify patients with probable advanced fibrosis who may benefit from hepatology or gastroenterology consultation.2