ImageJ software was used to analyze the C-arm radiographs. Measurements were divided into 4 groups of joint surface loss caused by the resections: 0% to 20%, 20% to 40%, 40% to 60%, and >60%. Differences in ROM between the BP and AS constructs were analyzed with a Wilcoxon signed rank test with statistical significance set at P < .05 (Prism 6; GraphPad Software).
Results
As many as 6 serial resections were made before the proximal fragment of the olecranon was judged too small to be secured to a plate with at least 2 screws. Only 7 specimens were large enough for the fifth cut, and only 4 were large enough for the sixth cut. After the final resection, mean loss of olecranon length was 77.3% (range, 63.7%-88%; median, 80.6%). All elbow specimens remained stable to manual valgus and varus testing in full extension, 30° of flexion, and full flexion in both supination and pronation. There was no medial or lateral opening of the ulnohumeral joint on fluoroscopy throughout testing, for either the BP or the AS constructs. There was no anterior or posterior subluxation throughout the entire ROM.
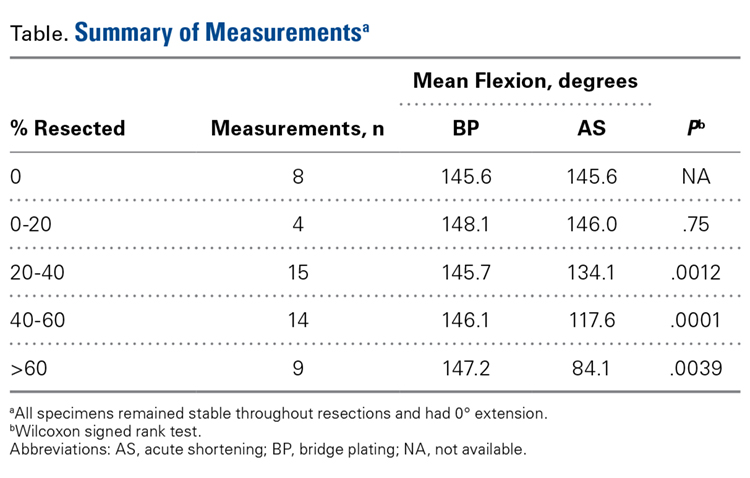
Table.
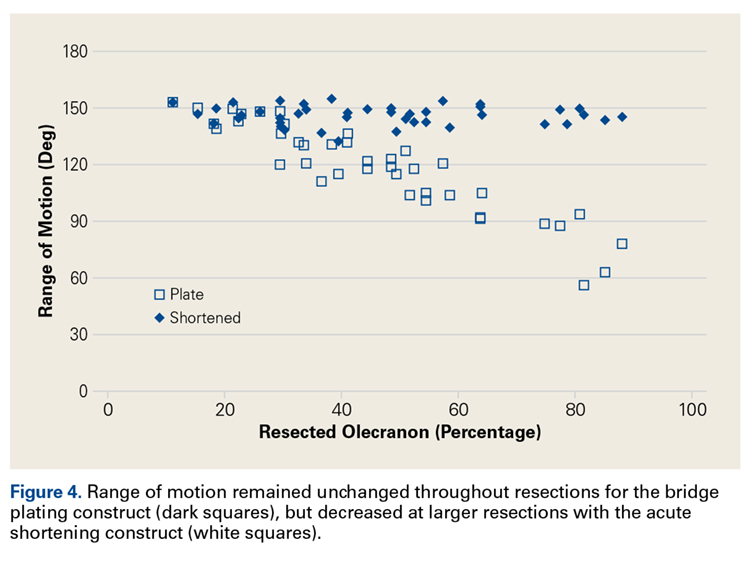
Mean extension was 0° initially and did not change over resections in both BP and AS constructs. Mean initial flexion for intact specimens was 145.6° (range, 146°-148°). In the BP constructs, flexion remained relatively unchanged (mean, 146°; range, 135°-155°) throughout testing. With increased resection of the olecranon, there was a significant decrease in flexion in the AS constructs. In AS, flexion decreased to a mean of 134° for 20% to 40% resection of the sigmoid notch, to 118° for 40% to 60% resection, and to 84° for >60% resection (Table). About 1° of flexion was lost for each 1% resection above 20% resection of intact length (Figure 4).