Each specimen was positioned with the arm draped in the lateral decubitus position, as in typical olecranon fracture surgery. A standard posterior approach to the olecranon was made with a midline posterior longitudinal skin incision. Subcutaneous flaps were developed, and the subcutaneous border of the proximal olecranon was exposed, preserving the medial and lateral collateral ligaments as well as the extensor mechanism. Baseline maximum flexion and extension of the elbow as well as olecranon length were measured with fluoroscopy (BV Pulsera, Philips) and ImageJ software (National Institutes of Health).
To ensure reproducible anatomical reduction during plating, a 3.5-mm 4-hole nonlocking periarticular anatomically contoured plate (Zimmer Biomet) was applied posteriorly to the intact olecranon through a longitudinal slit in the distal triceps tendon. The plate was predrilled to house 4 nonlocking screws, 2 proximal and 2 distal.
Fracture Generation and Testing of Fixation Constructs
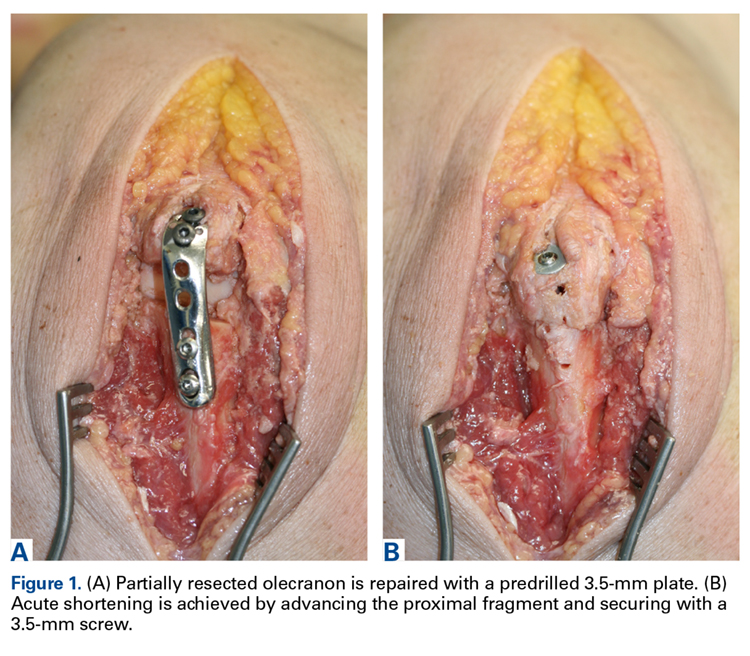
Figure 1.
Comminuted olecranon fractures were simulated by resecting a portion of the bone using an oscillating saw with a blade 2 mm thick. Resections were made perpendicular to the dorsal apex of the sigmoid notch under fluoroscopy guidance and were performed off the proximal and distal fragments interchangeably. At each resection, the specimen was repaired with the predrilled 3.5-mm BP and later with an AS construct (Figures 1A, 1B). For AS, the proximal fragment was advanced to the distal fragment and secured with a 3.5-mm screw, with the near cortex overdrilled to create a lagging effect. The resected surfaces of the olecranon were beveled without changing intra-articular length, and the proximal fragment was positioned to create a congruous surface for articulation with the trochlea. Both fixation methods, BP and AS, were used for each specimen at each resection. Serial resections were continued until the proximal fragment was too small for adequate fixation with 2 screws.
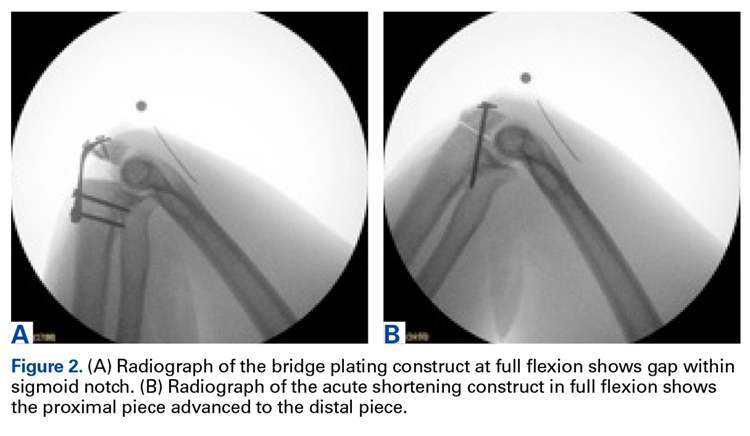
Figure 2.
After each fixation, radiographs were taken for measurement of maximum flexion and extension and amount of olecranon removed (Figures 2A, 2B). Gross stability to valgus and varus stress was examined under fluoroscopy after fixation, as it would be performed during surgery using manual valgus and varus load in full extension, 30° of flexion, and full extension in both supination and pronation. Any ulnohumeral joint line opening relative to baseline was considered a sign of instability.24
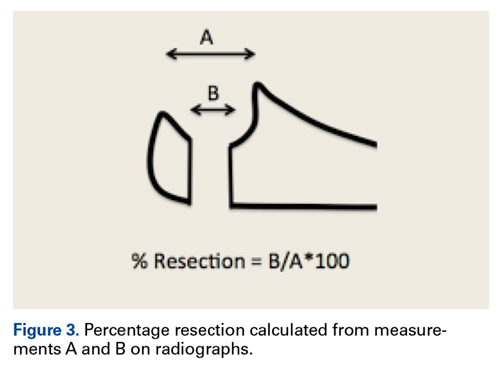
Figure 3.
On each radiograph, a marker was used to account for magnification artifacts. ROM was measured using the angle subtended by the longitudinal axis of the humeral shaft referenced by the anterior border of the humerus, and the longitudinal axis of the ulnar shaft referenced by the dorsal border of the ulna. The simulated fracture gap was measured at the articular surface. The articular surface length, measured before the resections, was used to calculate the percentage of the resected olecranon at each serial resection (Figure 3).