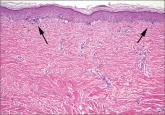
A diagnosis of Grover’s disease is usually made clinically based on the appearance of the rash and the patient’s age and sex (typically seen in middle-aged men). The diagnosis can be confirmed by biopsy. Under a microscope, Grover’s disease has a characteristic appearance of acantholytic dyskeratosis (FIGURE 2); it can be similar in appearance to Darier’s disease, Hailey-Hailey disease, or pemphigus.7
There are no curative treatments for Grover’s disease. Treatment usually is symptomatic. Local application twice a day of topical steroids, such as triamcinolone acetonide or fluticasone propionate, is often used to relieve the itching and reduce inflammation. Oral steroids, oral retinoids, calcipotriol, phototherapy with ultraviolet B or psoralen plus ultraviolet A light, Grenz radiation, and methotrexate may help clear the eruption in patients with severe itch or extensive or refractory disease.3,8 Antibiotics such as topical fucidin 2 to 3 times a day or oral cloxacillin 500 mg 4 times a day are indicated only if there is secondary impetiginization.
Advise patients to avoid excessive sweating, excessive sun exposure, occlusive clothing, and contact with topical irritants because all of these things are likely to make an outbreak worse.
Our patient was instructed to apply a topical clobetasone butyrate 0.05% cream twice a day. He was also told to take an oral antihistamine, fexofenadine, 180 mg bid for 2 months. The lesions healed, leaving hyperpigmentation. He was advised that the lesions might return in the future.
CORRESPONDENCE
Ch’ng Chin Chwen, MBBS, MRCP, Department of Medicine, Faculty of Medicine, University of Malaya, Lembah Pantai, 50603 Kuala Lumpur, Malaysia; chinchwen@gmail.com