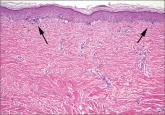
A clinical diagnosis of Grover’s disease (transient acantholytic dermatosis) was confirmed by skin biopsy.
First described in 1970,1 Grover’s disease is characterized by a monomorphic papulovesicular eruption that is limited to the trunk and is seen mainly among middle-aged2 Caucasian men.3 Most cases of Grover’s disease are benign and self-limiting, lasting weeks to months, but it can be difficult to manage and has been reported to be recurrent or persistent.4
Some researchers have proposed that Grover’s disease is caused by obstructed sweat glands that lead to pooled sweat urea coming out of the epidermis, resulting in acantholysis.5 However, patients typically present during the winter months when presumably they perspire less frequently.2
There is some evidence linking infection, infestation, ionizing radiation, drugs such as sulfadoxine/pyrimethamine, and recombinant human interleukin-4 with the development of Grover’s disease;3 however, the evidence is weak. Patients with recurrent Grover’s disease often report a history of asteatotic eczema, atopic dermatitis, or contact dermatitis.3
Because the clinical features of Grover’s disease are often subtle (macules and papules are not florid) and variable (may be red or brown and usually papular but can be acneiform, vesicular, pustular, and even bullous), diagnosis requires a high degree of clinical suspicion. There are many potential differential diagnoses, including:
Truncal acne may present as inflammatory papules. Patient may complain of itchiness. Comedones and pustules are telltale signs of truncal acne, and are not present in Grover’s disease.
Seborrheic dermatitis often presents as greasy, scaly, eczematous patches, and papules. It can be found on the hair-bearing area on the scalp, forehead, eyebrows, nasolabial folds, postauricular skin, and anterior chest wall. Grover’s disease typically presents on the trunk.
Folliculitis may look very similar to Grover’s disease, and its erythematous papules are often found on the trunk. Distinguishing the 2 can be done on biopsy.
Exanthematous drug eruptions, also called maculopapular eruptions, are not limited to the trunk. They are often associated with the use of a new medication within the previous 4 to 21 days.6