Falls risk: Make use of assessment tools
Each year, approximately 30% to 40% of elderly adults living independently fall, and the incidence increases with age.4 Falls frequently cause injuries, such as hip fractures, and reduce HRQoL.24 Strong evidence supports the efficacy of a multifaceted approach for identifying and reducing risk of falls in this patient population.25,26 A review of more than 3000 falls indicated that about one-third were the result of accidents or environmental hazards, and nearly another third were caused by gait problems, balance disorders, or weakness.27
Means of determining risk of falls. As with hearing assessment, you can gauge older patients’ risk of falls during routine visits or annual exams. For patients’ first Medicare visit, the AAFP Medicare preventive exam encounter form17 includes 2 items in the “Functional Ability/Safety Screen” section that cover the leading causes of falls. Item 1 asks, “Was the patient’s Timed Up & Go test unsteady or longer than 30 seconds?” This simple test requires patients to stand from a sitting position, using their arms for support; walk a few paces, turn around, and return to their chair to sit. The test is sensitive to, and specific for, identifying elderly people living independently who are at risk of falls.28
The Dizziness Handicap Inventory–Screening version (DHI-S) (FIGURE 2),29 is a 10-item patient self-assessment questionnaire that takes fewer than 5 minutes to complete. You can also use the DHI-S to supplement the Timed Up & Go test in judging a patient’s postural control.
Possible reasons for poor performance on the Timed Up & Go test are vestibular dysfunction or other balance disorders that require a careful evaluation. Cross-checking the “Medications, supplements, and vitamins” list in the “Medical/Social History” section of the Medicare encounter form may reveal use of a drug or multiple drugs (particularly likely if the patient sees different physicians) that commonly contribute to falls.30
Patients’ descriptions of “Past personal illnesses and injuries,” also covered in the encounter form, or their accounts of situations that provoked dizziness, may help you identify the presence of a disorder such as benign paroxysmal positional vertigo, which increases the risk of falls.31
In weighing whether to treat such a disorder yourself or to refer, keep in mind that the evidence strongly supports the efficacy of referring patients to otolaryngologists or audiologists for further diagnosis and treatment.32 Vestibular rehabilitation is effective for elderly patients with stable but symptomatic and uncompensated central deficits.33
FIGURE 2
Dizziness Handicap Inventory-Screening version (DHI-S)
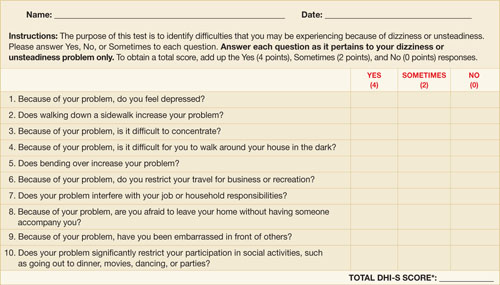
Source: Jacobson GP, et al. Am J Otol. 1998.29 Reprinted with permission.
*The higher the score, the greater the need for further evaluation.
Item 3 on the AAFP Medicare encounter form17 probes for hazards in the home, asking: “Does your home have rugs in the hallway, lack grab bars in the bathroom, lack handrails on the stairs or have poor lighting?” Strong evidence supports the efficacy of a home hazard assessment and modification in preventing falls. However, during the brief time allotted for an office visit, asking patients to recall and describe every potential hazard in their homes is impractical. The PATIENT HANDOUT (HOW TO REDUCE YOUR RISK OF FALLS) details the causes of falls in older people and preventive measures that patients or their families may be able to implement at home.
How to reduce your risk of falls
Injuries from a fall can range from bruises and cuts to more serious problems, like a broken hip. Fortunately, most falls can be prevented. If you’ve fallen recently or think you might have a balance problem, tell your doctor immediately.
Am I in danger of falling?
People fall more as they get older because of changes that come with age, such as poor vision, balance problems, weak muscles, and arthritis. Cluttered, poorly lit living quarters also increase the risk. You are more likely to fall if you:
- have fallen before
- don’t get much exercise and have weakness in your legs
- are unsteady when you walk
- are taking medicines that can contribute to falls, such as sedatives or antidepressants, or take 4 or more different medications
- have medical problems such as Parkinson’s disease, osteoporosis, heart disease, or low blood pressure—or if you have had a stroke.
How can I protect myself at home?
You can minimize the risk of falling at home by taking these steps:
- Keep the floors free of clutter. Remove things you can easily trip over, such as throw rugs, electrical cords, piles of paper, and clothing.
- Make sure you have good lighting throughout the house, and put night lights in your bedroom, bathroom, hallways, and stairs.
- Have railings installed in the bathtub and shower and around the toilet, and use nonskid mats in the tub and shower area.
- Keep items within easy reach in the kitchen.
- Put handrails on the stairs. (Using bright paint or strips of tape on the railing will make it easier to see.)
- Wear shoes with firm, nonskid soles. Don’t wear house shoes, such as flip-flops or loose slippers, or shoes with heels higher than 1 inch.
What else can I do to protect myself?
- Get your eyes checked regularly. Wear your glasses as prescribed, and clean them often to improve visibility.
- Stay active and exercise often to keep your muscles and bones strong. Ask your doctor about weight-bearing exercise, and what you can do to improve your balance.
- Eat a healthy diet, with plenty of calcium and vitamin D. Limit consumption of alcoholic beverages (have no more than 2 drinks a day).
- Take care of your feet. If they hurt, tell your doctor.
- Ask the doctor whether you need a cane or other walking aid.
- Have your doctor go over all your medicines to see if you’re taking anything that can make you dizzy or sleepy.
- Get up very slowly. When you’re getting out of bed, sit on the side for a few minutes before you stand up. Getting up too quickly can make you feel dizzy or lose your balance.
- If you live alone, get an emergency alert system that you can wear around your wrist or neck and press to call for help if you fall and can’t reach the phone.
Where can I get more information?
American Geriatrics Society
212-308-1414
http://www.americangeriatrics.org
National Center for Injury Prevention and Control
770-488-1506
http://www.cdc.gov/ncipc/falls/#PDF
National Institute on Aging
http://www.niapublications.org/engagepages/falls.asp
U.S. Consumer Product Safety Commission
http://www.cpsc.gov/CPSCPUB/PUBS/701.html
Sources: Rao SS. Am Fam Physician. 20054; Tremblay KR, et al. Colorado State University. 2005.34