A time-saving suggestion. You can save precious consultation time by having elderly patients complete a standardized self-assessment questionnaire such as the Hearing Handicap Inventory for the Elderly-Screening version (HHIE-S) (FIGURE 1) while they’re in the waiting room.18,19 When hearing loss is identified, counsel the patient as appropriate and strongly recommend further audiologic testing and management.20 The HHIE-S can help patients realize the social and emotional consequences of hearing loss, which may encourage them to seek assistance. But many won’t do so without your recommendation.
Let patients know something can be done. Evidence shows that nonmedical management of sensorineural hearing loss, including the fitting of hearing aids, is critical in helping older adults improve communication and reduce psychosocial problems.10,21
Recently, a task force of the American Academy of Audiology conducted a systematic review of the HRQoL benefits of amplification in adults.21 A meta-analysis revealed that hearing aids had at least a small effect on HRQoL, as measured by generic health instruments (eg, the Medical Outcomes Study Short Form-36), and medium-to-large effects when disease-specific hearing outcome measures (eg, the HHIE) were used. Hearing aids, combined with auditory rehabilitation, changed patients’ perception of their handicap to a greater extent than amplification alone, particularly during the initial stage of adjusting to a device.22,23
Preprinted forms can help educate patients about hearing loss and the benefits of amplification. The PATIENT HANDOUT (ARE YOU HAVING HEARING PROBLEMS?) explains the causes and symptoms of sensorineural hearing loss, as well as diagnosis, frequency of audiologic evaluations, and treatments.
Are you having hearing problems?
Sensorineural hearing loss occurs when sensory receptors (hair cells) in the inner ear (cochlea) or hearing nerve pathways to the brain are damaged. It is usually permanent and cannot be treated medically or surgically, but hearing aids almost always help.
Hearing loss most commonly results from age-related changes in the inner ear. Other possible causes are excessive noise exposure, drugs that are toxic to the auditory system, certain viruses or diseases, head trauma, and genetic or familial disorders.
If you think you may have a hearing loss or are having difficulty communicating, tell your doctor immediately.
What are the signs that I may be losing my hearing?
You may:
- complain that people are mumbling
- continually ask people to repeat themselves
- avoid noisy rooms, social occasions, or family gatherings
- prefer the TV or radio louder than other people do
- have difficulty understanding people when you can’t see their faces
- have trouble hearing at the movies or theater, your house of worship, or other public places
- have difficulty following conversations in a group
- become impatient, irritable, frustrated, or withdrawn.
Why can I hear people talk but not understand what they’re saying?
Hearing loss not only reduces your ability to hear normally audible sound, it interferes with your ability to detect particular sounds. High-pitched consonants (such as d, f, sh, s, t, and th) become harder to hear than low-pitched vowels. The high-pitched consonant sounds carry the meaning of words and help us understand speech, but in normal conversation, they’re softer than the less important low-pitched vowel sounds. So conversation may sound loud enough, but the words may not be clear.
How is hearing loss diagnosed?
Audiologists—health care professionals who specialize in hearing—conduct a comprehensive evaluation to determine the degree and type of hearing loss and its effect on your ability to communicate in everyday life. The exam is conducted with special instruments in a sound-dampened room. Medical diagnosis of ear disease is performed by ear, nose, and throat doctors (also known as ENTs or otolaryngologists).
How often should I have a hearing test?
After age 50, you should have your hearing tested every 2 years. But it’s important to request a hearing test immediately if you notice a sudden change in hearing, increased ringing in the ears (tinnitus), or dizziness.
How is hearing loss treated?
Hearing aids, which work better than ever because of digital technology, help many people. Your audiologist will talk to you about the different kinds of hearing aids available and what you can realistically expect when you use them. Together you’ll decide which one is best for you.
People who use hearing aids report better personal relationships, an easier time communicating, improved mental health, and a greater sense of control over their lives.
Where can I get more information?
American Academy of Audiology
800-AAA-2336
http://www.audiology.org
American Academy of Otolaryngology, Head, and Neck Surgery
703-836-4444
http://www.aaohns.org
American Speech-Language-Hearing Association
800-638-8255
http://www.asha.org
FIGURE 1
Hearing Handicap Inventory for the Elderly—Screening version (HHIE-S)
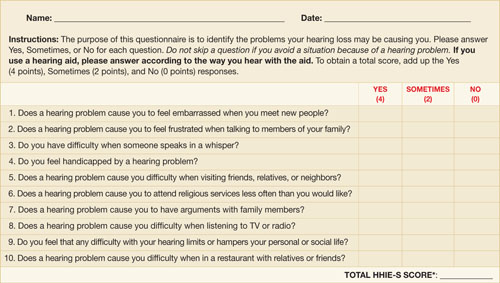
Source: Ventry IM, et al. ASHA. 1983.18 Reprinted with permission.
Copyright 1983 by American Speech-Language-Hearing Association. All rights reserved.
*If your score is 10 or greater, you may benefit from additional hearing evaluation.