Gary Rivard, DO Anthony Viera, MD Family Medicine Residency Program, Central Maine Medical Center, Lewiston (Dr. Rivard); Department of Family Medicine, University of North Carolina at Chapel Hill (Dr. Viera) rivardga@cmhc.org
The authors reported no potential conflict of interest relevant to this article.
Tx IS EFFECTIVE WHEN STARTED EARLY Antibiotics are an effective treatment for pertussis, but they need to be started within the first few weeks of developing symptoms. Studies have not found evidence that antibiotics shorten the duration of pertussis symptoms unless they are given in the catarrhal phase.22,23 It can be challenging to get treatment started during this window, however, because patients may put off seeking care for symptoms they perceive as only minor, such as a cough, until the disease progresses. In addition, physicians may not suspect pertussis in patients who present with a cough they have had for only a short time, and therefore may not test for it.
It may be necessary to rely on clinical suspicion when deciding whether to initiate treatment for pertussis before testing to confirm the diagnosis. For patients in whom clinical suspicion of pertussis is high and who may be in contact with high-risk individuals, it may be acceptable to begin treatment before receiving lab test results.24,25 A recent Cochrane meta-analysis26 recommended initiating treatment to render a patient who has pertussis “noninfectious” but without an expectation of diminishing symptoms.
Limited role for prophylaxis. There is little evidence that prophylactic treatment for pertussis can decrease the spread of the disease. Studies that investigated potential benefits of prophylactic treatment for pertussis have been inconclusive, except for individuals who are in close contact with an infant younger than 6 months of age who has not been fully immunized.27,28
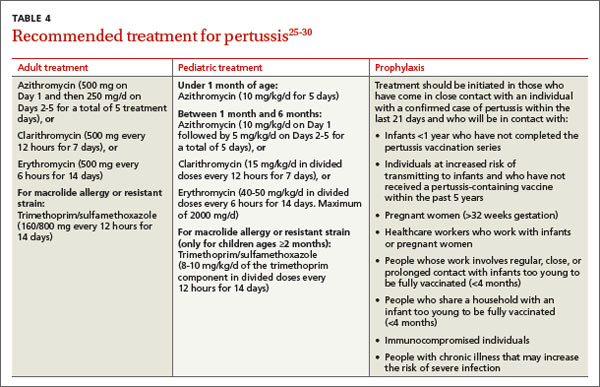
A macrolide antibiotic is generally used to treat pertussis (TABLE 4).25-30 Consider starting treatment before lab results are in when clinicial suspicion is high and the patient may be in contact with high-risk individuals. Erythromycin had been the drug of choice, but recent studies have found similar efficacy for azithromycin and clarithromycin.29 For infants younger than one month of age, azithromycin is preferred because in addition to being as effective as other macrolides, it has a better adverse effect profile.29 For patients who are at least 2 months of age, trimethoprim-sulfamethoxazole is an acceptable alternative to a macrolide.
The CDC recommends that any adolescent or adult who has a cough and has had close contact with an individual with a laboratory-confirmed case of pertussis within the past 21 days should be treated.30 Close contacts younger than 7 years of age who have not received the first 4 doses of the pertussis vaccine should be offered treatment.
CORRESPONDENCE Gary Rivard, DO, Family Medicine Residency Program, Central Maine Medical Center, 76 High Street, Lewiston, ME 04282; rivardga@cmhc.org