Authors’ Disclosure Statement: Dr. Hirahara reports that he receives support from Arthrex as a consultant, royalties, and research support. Dr. Panero reports no actual or potential conflict of interest in relation to this article.
Ultrasound allows the surgeon to localize any superficial foreign objects, especially with radiolucent objects like fragments of glass. Small glass fragments or pieces of wood have always been extremely difficult to remove. X-rays cannot localize these objects, so getting a proper orientation is difficult. MRI and CT scans easily identify these types of foreign objects, but cannot be used intraoperatively (Figure 1A). Often, these objects cannot be felt and therefore require a large dissection. The objects may encapsulate and be easily confused with other soft tissues.
These objects often take large incisions and wide dissections to find and remove. With ultrasound, the objects can be localized in real time while in surgery(Figure 1B).Using a sterile probe cover, the surgeon can take advantage of the multi-planar nature of ultrasound. Since the probe can be manipulated in any direction and angle, the only limitations to finding objects are the user, the object density, the location depth, and if the object is behind a hard structure, such as bone. The foreign body can then be removed under ultrasound guidance (Figure 1C).Being able to identify specific structures in surgery allows the surgeon to be more accurate when performing certain procedures. Arthroscopic biceps tenodesis is a common shoulder procedure that can be done many different ways. When using the “below the groove/supra-pec” position, the incisions become more variable and difficult to place. If the surgeon is too high/low or medial/lateral, the localization of the drill position will be very difficult, which will result in having to angle the drill to compensate for poorly placed portals, and finding the biceps becomes very challenging.
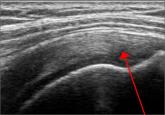
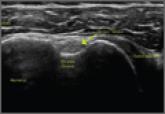
By using the ultrasound intraoperatively, the surgeon can identify the exact position of the biceps tendon (medial/lateral) and where it lies just below the groove and above the pectoralis major (superior/inferior) (Figure 2A).
This allows the surgeon to mark the appropriate placement of the portals by the position of the transducer (Figure 2B). When entering with the arthroscope to perform the procedure, the surgeon will “fall” right onto the biceps tendon at the exact level needed to perform the tenodesis. This is not just more accurate, but safer, as it will not endanger any nerves or vessels.
Reconstruction of ligaments is another ideal use of ultrasound. Surface anatomy cannot always tell the exact location of a ligament or tendon insertion. The best example of this is the anterolateral ligament (ALL). Identification of the lateral epicondyle of the femur and anatomic insertion of the ALL can be difficult in some patients. Ultrasound can be used to identify the origin and insertion of the ALL during surgery under sterile conditions (see page 418). A spinal needle can be placed under direct vision with an in-plane ultrasound guidance over the bony insertion (Figure 3A). A percutaneous incision is made.
The spinal needle is replaced with a guide wire and drilled into place (Figure 3B). A cannulated drill of appropriate size is used to create the socket or tunnel. In the case of the ALL, a 5.0-mm diameter reamer is used to a depth of 22 mm at both the origin and insertion. A 4.5-mm semitendinosus graft is prepared with a collagen-coated FiberTape (Arthrex) attached to a 5.5 BioComposite Vented SwiveLock (Arthrex). It is attached proximally, buried under the iliotibial band (ITB) and then attached distally with the knee in 40° of flexion with a second 5.5 BioComposite Vented SwiveLock. The FiberTape is used as an internal brace to allow for early motion and weight-bearing.
This technique is also used by the senior author (AMH) to repair, reconstruct, or internally brace the medial collateral ligament, medial patellofemoral ligament, and lateral collateral ligament. This technique is ideally suited to superficial ligament and tendon reattachment, reconstruction, or internal bracing. The knee, ankle, and elbow superficial ligaments are especially amenable to this easy, percutaneous technique.
Conclusion
Ultrasound is quickly becoming a popular imaging modality due to its simplicity, portability, and cost efficiency. Its use as a diagnostic tool is widely known. As an adjunct for procedures and interventions, its advantages over larger, more expensive modalities such as fluoroscopy, CT, or MRI make it stand out. Ultrasound is not the perfect solution to all problems, but it is clearly a technology that is gaining traction. Ultrasound is another imaging modality and tool that physicians and surgeons can use to improve their patients’ treatment.