"I am I plus my circumstances."
Flying from Boston to San Diego, next to me was a man in his 40s or 50s. A summer downdraft dropped the floor of the plane precipitously.
“Oh, my,” I said out loud.
“Roger that,” my row mate said.
With the social silence broken, he asked if I were leaving or returning, for business or pleasure, and what I did for a living.
“Physician, psychiatrist. And you?”
“Electrical engineer. I design heads-up displays for fighter-bomber aircraft cockpit simulators. What kind of psychiatry? Medication? Talk?”

Dr. Neal A. Kline
“Posttraumatic stress disorder. Inner city. Talk and medication. However, many of the people I see would rather not participate in talking therapy and not take medication, wishing impossibly to return to the life they were living before the traumatic event occurred. Here’s an example: I recently saw a woman in her late 30s. She told me of sitting on her stoop at home with her 14-year-old son. In a drive-by hail of bullets, her son was hit in the head and died at her feet. She was referred to me by her general physician who told her she was depressed. ‘Depressed,’ she repeated. ‘I don’t eat or sleep. I don’t go outdoors if I can avoid it. And I put my hands over my ears if I hear a siren outside. But I don’t want therapy, and I don’t want medication. I want my son back. I want my life to be the way it used to be.’ ”
“Like hysteresis,” the engineer said. “Hysteresis is a scientific term, from the Greek root meaning ‘late’ or ‘lagging behind.’ Hysteresis is about being changed and not being able to reverse the change. It’s being permanently changed by the changing event.”
Tearing out a page from his magazine and folding it in half, he said, “Unfold it.”
I complied.
“But what about the fold line?” he asked. “Can you return the paper to its unfolded state with no evidence of its having been folded? The paper has acquired and retained memory of being folded. There’s a residual line you cannot get rid of.”
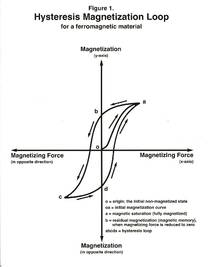
Then he drew for me a hysteresis-magnetization graph of an iron particle in a variable electromagnetic field. Starting at the origin (O), where the x-axis/horizontal and the y-axis/vertical intersect, he “pulled” the particle to the right using a hypothetical electromagnetic force, and graphed the rise of the iron particle’s magnetized state by its position on the vertical axis. But the graph was not linear. The iron’s magnetic induction lagged behind the force applied to it.
“It takes time and energy for magnetic molecular rearrangement, for magnetism to get started, so there’s a lag in the saturation curve.
“At the top of the curve, at magnetic saturation, if the magnetizing current is stopped, the curve does not trace itself back to the origin. Rather, it stays flat at the top, lagging, needing time and energy to disaggregate the magnetized molecular domains. Belatedly, the iron speck’s magnetization responds to the lack of current, with reduced magnetization, and follows an independent downward curve, crossing the y axis significantly above the origin, O (Figure 1).
 Courtesy Dr. Neal A. Kline
Courtesy Dr. Neal A. Kline
“This is the point of residual magnetization, the partial magnetization that remains from the full current from the past, now turned off – representing the iron’s ‘remembering’ its history.”
As the engineer drew his hysteresis magnetization curves, I looked over his shoulder and reframed, for sport, his terminologies from the upper right quadrant of his graph as follows: his “a,” “fully magnetized,” I changed to “fully traumatized”; “b,” his “residual magnetization” (magnetic memory), I changed to “residual traumatization” (memory of the trauma); and “o,” his “initial nonmagnetized state,” I changed to the “initial nontraumatized state,” to which the person never returns, that is, with no evidence of having been exposed to the traumatizing circumstance. However, his three other magnetization quadrants did not lend themselves to my “traumatic relabeling,” as conceptually there is no “traumatization in the opposite direction” or “traumatizing force in the opposite direction.” Indeed, rape has no antonym.
Our plane continued westward, crossing the Mississippi and the Grand Canyon while my new best friend and I examined one-way events, or entities, that could not be returned to their previous states once significant change had been made, no matter how diligent the efforts at remedy:
Humpty Dumpty…
Death…
Aging…
An insult, given or received…
First impression…
Surprise ending…
Snapped twig…
Popcorn…