Switching to an antipsychotic with relatively less histamine or alpha-adrenergic blockade may reduce problematic side effects such as sedation and orthostatic hypotension, respectively (Table 2).
Patients vary in how well they tolerate other side effects, such as weight gain. For example, a 10-lb weight gain may be acceptable to one patient and unacceptable to another. The decision to switch may be more obvious in a patient with diabetes, for whom substantial weight gain is unacceptable.
SWITCHING STRATEGIES
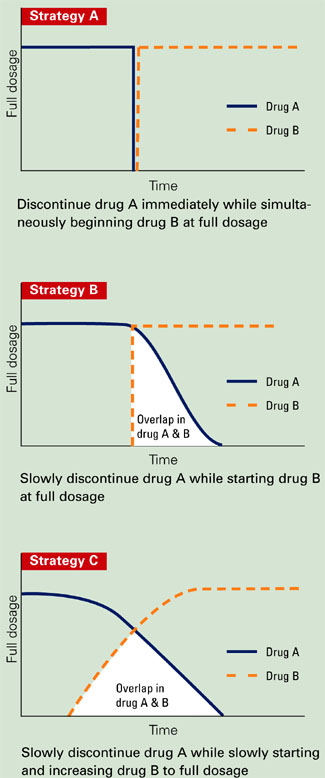
No method is universally accepted for switching from one antipsychotic to another. In clinical practice and research, three common methods (Figure) are used:
- immediately discontinuing drug A while starting drug B at full dosage
- slowly tapering drug A while starting drug B at full dosage
- slowly tapering drug A while slowly increasing drug B to full dosage.
Each method has advantages and disadvantages. Gradual cross-titration and tapering may reduce the risk of relapse but increase the risk of side effects. Elaborate regimens may confuse some patients—especially those with cognitive impairment—and increase the risk for adverse events and nonadherence.
Abruptly discontinuing an agent is less confusing and more convenient than gradual tapering, but patients may experience acute withdrawal (as with clozapine). Finally, no guidelines exist on how quickly to make the transition when one or both medications are cross-titrated and tapered. For inpatients receiving intense monitoring, a transition may be completed in 3 to 7 days, whereas outpatients may require 1 to 3 weeks.
Recommendation. The evidence cited in the next section of this article suggests that any of the three methods can be used when switching antipsychotics, except clozapine. When switching from clozapine, extend the cross-taper period to help minimize or eliminate rebound psychosis and cholinergic symptoms.
SWITCHING FROM DEPOT TO ORAL AGENTS
For patients switching from depot to oral antipsychotics, a 1-month cross-titration taper has been shown to be efficient and safe.
Godleski et al3 randomized 26 patients who had received IM depot antipsychotics (haloperidol or fluphenazine decanoate) for at least 3 years to either continue the IM depot antipsychotic or switch to olanzapine. Although the study was designed to assess the safety and efficacy of the switch, it also provided data on the transition method.
Figure 3 common antipsychotic switching strategies
Subjects switching to olanzapine received their routine depot injection plus olanzapine, 10 mg/d for 1 month, followed by olanzapine monotherapy (5 to 20 mg/d) for 2 months. Those who continued IM depot therapy were maintained at a stable dose and dosing interval for 3 months. Safety and efficacy data were collected at baseline and monthly.
Patients receiving olanzapine improved on several efficacy measures, although the clinical relevance was minimal. For example, their mean PANSS total score decreased 3.23 points. One patient—in the control group—was hospitalized. Those who received olanzapine preferred this agent to the IM depot formulations and chose to continue daily olanzapine therapy. Adverse events did not increase significantly while patients received IM depot injections plus olanzapine.
SWITCHING ORAL AGENTS
Clozapine. When risperidone entered the U.S. market in the 1990s, a number of patients who had been treated with clozapine were abruptly switched to risperidone. Many experienced acute symptom exacerbation,4,5 including some whose rebound psychosis was more severe than their original symptoms. Other adverse effects—including nausea, diarrhea, vomiting, headache, restlessness, and sweating— have been attributed to cholinergic rebound caused by abruptly discontinuing clozapine.
To minimize the potential for rebound psychosis and cholinergic symptoms, taper clozapine across a minimum of 1 to 2 weeks. When you need to discontinue clozapine immediately—such as for patients experiencing serious hematologic effects—adding an anticholinergic such as benztropine may minimize the cholinergic rebound.
Risperidone. No studies have formally assessed methods for switching patients to risperidone.
Olanzapine. When switching to olanzapine, a direct switch or cross-titration tapering appear to be viable options.
In one multicenter, open-label study,2 108 patients were randomly assigned to olanzapine, 10 mg/d, after abruptly discontinuing a previous antipsychotic (direct switch) or by cross-titration tapering in a 1:1 fashion. Patients in the crosstitration group started olanzapine and discontinued their original antipsychotics across 2 weeks. Olanzapine dosages were adjusted as needed from 5 to 20 mg/d.
At study entry, approximately 95% of subjects in the direct-switch group and 85% in the crosstitration taper group were taking at least one typical antipsychotic—usually haloperidol. A switch was considered successful if a patient completed the 6-week trial without psychotic symptom worsening or EPS.
The 92 (85%) subjects who completed the study comprised similar percentages from both groups. Their scores on the PANSS total and subscales and Clinical Global Impression (CGI) scale also were similar.