Combination therapy is another type of OLP. Often a disease state consists of multiple underlying syndromes, and treating individual syndromes is a common strategy. For example, in addition to depressed mood, a patient with major depressive disorder also may have insomnia and poor concentration. A medication approved for treating depressed mood may not improve insomnia or poor concentration. Therefore, combination therapy may be necessary, but likely would be off-label. Combination therapy also may be tried when a patient does not respond to monotherapy. For example, although the evidence supporting the practice is inconclusive, clinicians commonly prescribe >1 antipsychotic to patients with schizophrenia or other psychotic disorders.
Help for making OLP decisions
Position statements/policies. The American Psychiatric Association (APA) and the American Medical Association support OLP when the practice is based on sound scientific evidence and medical opinion.11 The APA position statement encourages clinicians to use various compendia, including the American Hospital Formulary Service (AHFS) Drug Information, in conjunction with peer-reviewed literature to determine the medical acceptability of off-label uses.11
Evidence-based medicine includes a hierarchy of scientific and clinical evidence that can justify medical decisions. At the top of this hierarchy are large RCTs and smaller RCTs; cohort studies, case-control studies, poorly controlled or uncontrolled studies, case reports, and expert opinion are less valuable (Figure 2).4
Searching through all available resources for evidence supporting a specific off-label use is a cumbersome, time-consuming process. For this reason, clinicians may refer to compendia that evaluate and rate the available evidence supporting off-label use of medication, such as the AHFS Drug Information and DrugDex. Other resources include peer-reviewed medical journals. Physicians can contribute to knowledge of off-label uses by sharing their experiences, both good and bad, with their colleagues via presentations, publications, and/or initiating a study.
Other resources. Gazarian et al12 delineated 3 situations where OLP might be considered appropriate: use justified by high-quality evidence, use in research trials, and exceptional use justified by individual clinical circumstances. Exceptional use would require all of the following:
- the patient has a serious disease or condition
- evidence supports a potential beneficial effect of the off-label treatment
- potential benefits outweigh potential risks
- standard therapy has failed or is inappropriate
- an institutional drug committee approved the off-label use
- the patient provides written informed consent.12
Other authors13,14 have offered recommendations for psychiatrists considering OLP:
- Study available literature and assess whether sufficient evidence supports the proposed off-label use.
- If evidence is lacking, learn about the medication and its potential risks (interactions, adverse effects, and FDA “black-box” warnings). Also consult other resources for additional information and research, including peers and experts in the field.
- Consider and document risks and benefits of the proposed off-label use. Explain these, as well as uncertainties and potential costs, to patients and/or their families, and obtain and document informed consent.
- Cautiously initiate the off-label therapy, monitor patients closely, and meticulously document efficacy and tolerance.
Prescribing medications on-label does not guarantee safety or efficacy. Likewise, OLP does not imply a safety hazard or lack of efficacy. OLP may be in the best interest of the patient. Nonetheless, the practice must be carried out responsibly with utmost caution and consideration of acute and long-term burdens to patients, along with an assessment of the risk vs benefit of the proposed therapy.
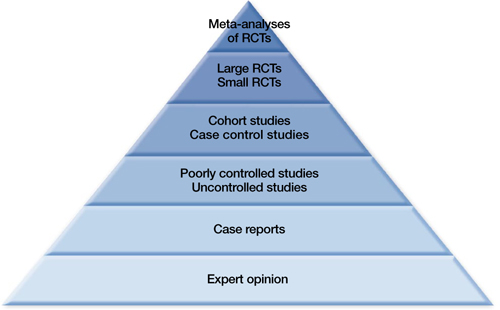
Figure 2: The hierarchy of sources for evidence-based medicine
RCTs: randomized controlled trials
Source: Reference 4Related Resource
- Mossman D. Why off-label isn’t off base. Current Psychiatry. 2009;8(2):19-22.
Disclosures
Dr. Ali receives research/grant support from Cyberonics and is a speaker for Merck.
Dr Ajmal reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.