Consulting psychiatrist’s role. If a patient is not sufficiently improved after 8 to 10 weeks, the care manager works with the PCP and psychiatrist to change treatment according to an evidence-based algorithm (Figure).12 In large health care systems, the psychiatrist meets weekly with the care manager to review treatment plans for approximately 100 depressed older adults, with particular attention to those who are not improving. Psychiatrists may see patients in person or facilitate other specialty mental health treatment, as indicated.
Patients are encouraged to choose an antidepressant prescribed by their PCP, psychotherapy provided by the care manager in the primary care setting, or both. The patient and PCP make treatment decisions with support from the care manager and psychiatrist.
After depressive symptoms remit, the care manager completes a relapse prevention plan with the patient. This includes:
- steps the patient can take to prevent a relapse
- identifying relapse warning signs
- an action plan if depressive symptoms recur.
Training for clinicians in the IMPACT model is available at workshops and on the Internet (see Related resources). Successful implementation requires addressing operational and financing issues, and potential funding sources for primary care-based management have been described.13
Figure 3-step IMPACT intervention for a typical older patient with depression
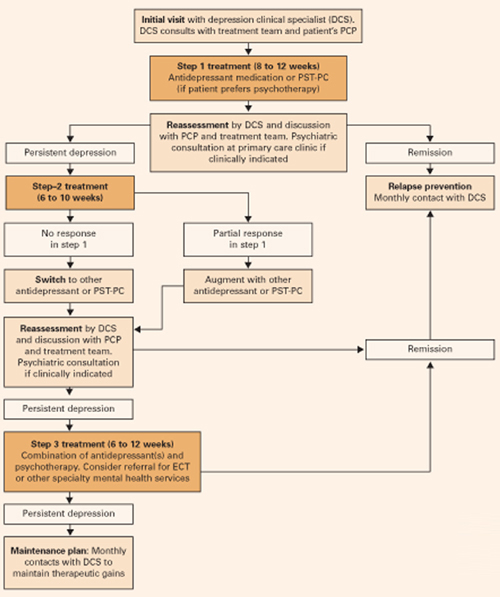
PST-PC: Problem Solving Treatment in Primary Care
ECT: Electroconvulsive therapy
Source: Adapted and reprinted with permission from Unützer J, Katon WJ, Williams JW, et al. Improving primary care for depression in late life: the design of a multi-center randomized trial. Medical Care 2001;39:785.
How impact was tested
The IMPACT team care model has been tested in a randomized trial with 1,801 depressed older adults from 18 primary care clinics in 8 U.S. health care organizations. These included feefor-service plans, health maintenance organizations, and Veterans Affairs clinics with more than 450 PCPs in rural and urban settings.
Patients were randomly assigned to receive IMPACT care for 12 months or care as usual (in usual care, the patient and provider were informed that the patient met diagnostic criteria for major depression or dysthymia). Patients assigned to usual care could engage in any depression treatment the provider normally used, including referral to specialty mental health services.14
Result: Better outcomes. IMPACT was more effective than usual care for late-life depression in all 8 organizations over 2 years.15,16 Overall, IMPACT doubled the effect of usual care. IMPACT patients:
- experienced >100 additional depression-free days17
- showed substantial improvements in physical and social functioning15,17 and quality of life,15 even 12 months after IMPACT resources were withdrawn18
- experienced less pain and pain-related functional impairment19
- had significantly less suicidal ideation.20
IMPACT care also was more cost-effective than usual care for depression in older adults with and without comorbid medical illnesses.17
From research to practice
Based on the robust study outcomes, researchers received a grant from the John A. Hartford Foundation to provide materials, training, and technical assistance to organizations interested in adopting IMPACT. More than 20 health care organizations have used IMPACT, and several have completed program evaluations showing outcomes matching the original IMPACT trial’s.
Kaiser Permanente of Southern California serves 3 million members. Before adopting collaborative care for depression, Kaiser conducted a pilot study of the project IMPACT model modified to fit its health care system. Adaptations included:
- expanding the program to serve depressed adults of all ages
- adding medical assistants to the care team to help with patient follow-up
- adding a “depression class” to offer group-based patient education
- providing psychiatric consultation to the care manager and primary care providers by telephone.
Kaiser investigators compared the outcomes of 300 patients who experienced the adapted program with outcomes in 140 usual-care patients and 140 intervention patients in the original IMPACT study. The effects on depression symptoms were equal to those achieved in the original IMPACT study, with 68% of depressed older adults showing substantial improvement (at least a 50% reduction in depression symptoms) at 6 months.21
- Project IMPACT. www.impact-uw.org.
- American Association of Geriatric Psychiatry. www.aagpgpa.org.
- Positive Aging Resource Center. http://positiveaging.org.
Acknowledgment
This paper is based on a presentation by Dr. Unützer for the Distinguished Scientist Award at the American Association of Geriatric Psychiatry annual meeting in Puerto Rico, March 10, 2006.