Anna D. Burke, MD Director Alzheimer’s and Memory Division Barrow Neurological Institute Clinical Assistant Professor of Psychiatry University of Arizona College of Medicine Clinical Assistant Professor of Psychiatry Creighton University School of Medicine Phoenix, Arizona
William J. Burke, MD Director Stead Family Memory Center Banner Alzheimer’s Institute Research Professor of Psychiatry University of Arizona College of Medicine Phoenix, Arizona
Disclosures Dr. Anna D. Burke reports no financial relationships with any company whose products are mentioned in this article, or with manufacturers of competing products. Dr. William J. Burke receives federal and state grants or research support from the Alzheimer’s Clinical Trial Consortium, Alzheimer’s Disease Cooperative Studies, Alzheimer’s Therapeutic Research Institute, and National Institute on Aging. He receives industry support to Banner Alzheimer’s Institute from AbbVie, AstraZeneca, Avid, Biogen, Eli Lily, Global Alzheimer’s Platform Foundation, Janssen, Merck, Novartis, Roche, and Suven. He is a consultant to Optum Labs and Otsuka Pharmaceuticals (Data Safety Monitory Board).
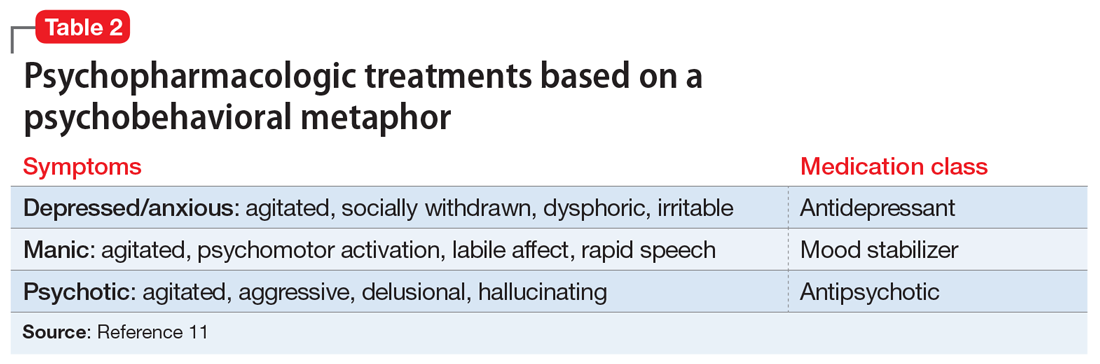
Alternative psychopharmacologic treatments based on a psychobehavioral metaphor should also be considered (Table 211). This approach matches the dominant target symptoms to the most relevant medication class.11 For example, in the case of a verbally and physically agitated patient who is also irritable, negative, socially withdrawn, and appears dysphoric, we might first undertake a trial of an antidepressant. Conversely, if the patient shows agitation in the context of increased motor activity, loud and rapid speech, and affective lability, we might consider the use of a mood stabilizer. Pharmacologic treatment should be aimed at the modification of clearly identified and documented target behaviors.
Indications to use antipsychotics for patients with dementia include:
severe agitation and aggression associated with risk of harm
Symptoms that do not usually respond to an antipsychotic include wandering, social withdrawal, shouting, pacing, touching, cognitive defects, and incontinence.12 These symptoms may respond to interventions such as changes to the environment.
Continued to: Choosing an antipsychotic
Choosing an antipsychotic
Once you have identified that an antipsychotic is truly indicated, the choice of an agent will focus on patient-related factors. Considerations such as frailty, comorbid medical conditions including diabetes, history of falls, hepatic insufficiency, cardiac arrhythmias, and cerebrovascular risk factors, should all be analyzed prior to initiating an antipsychotic. The presence of these conditions will increase the likelihood that adverse effects may occur. It will also guide the dose trajectory and the target dose for discontinuation. Antipsychotics differ with respect to their efficacy and adverse effect profile. For practical purposes, adverse effects typically guide the selection of these agents when used for patients with dementia.