
Clinician#2 inserts the balloon into the uterus by placing her hand into the vagina and guiding the balloon into the proper intrauterine position. (Most often, clinician#2 is the delivering clinician.) This technique is performed in a manner similar to how one places an intrauterine pressure catheter.5
Clinician #2 stabilizes the balloon in position by maintaining her hand in the vagina. She ensures that the balloon does not “pop” out of the lower uterus as the balloon is filled (FIGURE).
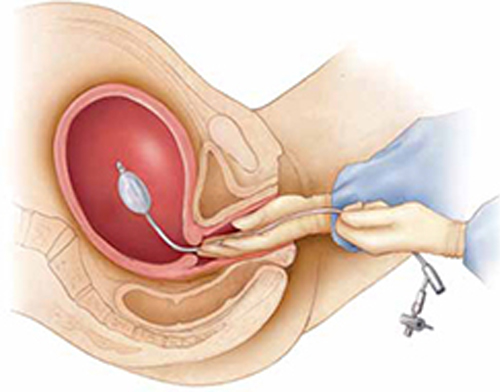
Manual insertion of a Bakri balloon
Insert the balloon into the uterus by 1) placing your hand into the vagina and guiding the balloon into the proper intrauterine position (similar to the manner in which an intrauterine pressure catheter is placed),5 2) stabilizing the balloon in position by maintaining the hand in the vagina, and 3) ensuring that the balloon does not “pop” out of the lower uterus as the balloon is filled.Clinician #3 simultaneously begins to instill sterile fluid into the balloon. This team member can be a nurse, medical assistant, or surgical technician.
My recommendation. Consider using simulation training to practice the team approach to placing the Bakri balloon. This is an effective method of improving team coordination.
TIP: Instill at least 150 mL of fluid
In short, use more fluid, not less. Although one study showed that most clinicians fill the balloon to a median volume of 300 mL,6 I’ve observed that some timidly instill the balloon with 80 to 120 mL of fluid. I think this is too little to maximize the effectiveness of the balloon for a postpartum patient who has massive hemorrhage.
Studies have shown that filling the balloon to at least 150 mL noticeably increases tamponade pressure.7
TIP: Place a pack in the upper vagina to stabilize the balloon in position
It usually takes only a few minutes after the Bakri balloon is filled to determine whether it is going to control uterine bleeding—what is called a tamponade test. If the balloon does control bleeding, you can place a vaginal pack of ribbon gauze to help ensure that the balloon does not slip down through the dilated postpartum cervix.
To avoid obscuring continued bleeding, however, do not place vaginal packing until you have obtained a positive tamponade test.
TIP: Check the hemoglobin concentration, platelet count, and coagulation status
The trauma literature demonstrates that optimal patient outcomes are realized when the following targets are maintained during resuscitation of patients who have massive hemorrhage8:
- hematocrit, ≥21%
- platelet count, ≥50 × 103/μL
- fibrinogen ≥100 mg/dL
- International Normalized Ratio (INR) ≤1.5.
These targets are achieved by appropriate transfusion of red blood cells, platelets, fresh frozen plasma, cryoprecipitate, and purified recombinant fibrinogen concentrate (RiaSTAP). Many trauma specialists recommend transfusion of a 1:1 ratio of RBCs and fresh frozen plasma in cases of major hemorrhage until coagulation status is normalized.
My recommendation. Often, it takes as long as 1 hour (sometimes, longer) to get results of Stat coagulation tests from the lab. While you are waiting, obtain clinical evidence of clotting function by filling a red-top tube with the patient’s blood. Adequate function is signaled by formation of a stable clot within 10 minutes.
TIP: Practice your team’s response to PPH with simulation
Last, I urge clinicians in every birthing unit to use simulation exercises to improve all facets of their response to severe postpartum hemorrhage.9
Summing up
Death following PPH remains a major cause of maternal mortality in developed and developing countries. The appropriateness of your response within 10 minutes of the onset of PPH is critical to ensuring a successful outcome and minimizing adverse events.10 To help, use the Bakri Postpartum Balloon often, and use it early.
We value your clinical insights!
What are your tips and tricks for effective use of intra-uterine balloon tamponade in postpartum hemorrhage?
To enter your response, click here or send your pearl to obg@qhc.com, with your name and location of practice.
We’ll publish a sampling of bylined contributions in an upcoming issue of OBG Management, with appreciation.