Remove the cervix, uterus, and adnexa (if planned) via the vagina. Close the vaginal cuff using laparoscopic suturing for appropriate cuff support.4
Supracervical hysterectomy. Level 2 is the endpoint. Begin at level 1 using reverse cone drilling (FIGURE 5). This will enable you to reach level 2. Then extract the uterus using the tissue morcellator.
Laparoscopic-assisted vaginal hysterectomy. Clamp, cut, and ligate the uterine vessels vaginally.
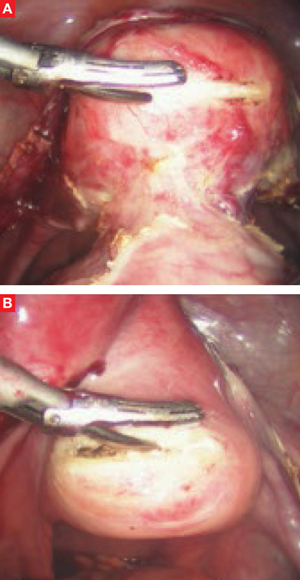
FIGURE 4 Anterior and posterior colpotomy
After the uterine vessels are secured and the 3 tissue levels have been identified, perform anterior (A) and posterior (B) colpotomy.
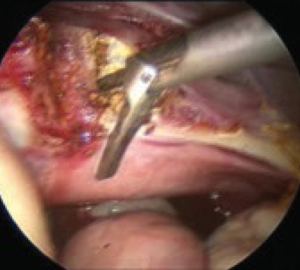
FIGURE 5 Supracervical hysterectomy
Begin the procedure at tissue level 1 using reverse cone drilling to reach the level 2 endpoint.
Always locate the ureter
Regardless of the type of hysterectomy being performed, it is critical to observe the ureter and ensure that it is out of harm’s way before securing the uterine vessels and identifying the tissue levels.
At the end of the procedure, always reduce intra-abdominal pelvic pressure to 5 mm Hg and check all tissue sites for hemostasis.
Not so long ago in the mid-1980s, we had fewer trocar options, laparoscopic suturing was limited, unipolar cautery was popular, endocutters could not guarantee hemostasis across staple lines, laparoscopes were large, images were unpredictable, monitors and cameras were nonexistent, and gas insufflators were bulky and slow. Despite these shortcomings, many surgeons and nurses believed minimally invasive surgery conferred advantages worth pursuing.
Then Semm pelviscopy (Kiel, Germany) reached the United States and intrigued American surgeons, both general and gynecologic.5 The ability to suture laparoscopically was crucial to the success of advanced operative laparoscopy.6 Laparoscopic cholecystectomy emerged, hastening further improvements in equipment and instrumentation.
Beginning in the late 1990s, laparoscopic surgeons witnessed even bigger changes in operating room technologies. The Internet increased the patient’s understanding of her options, and this new awareness motivated hospitals, industry, and physicians to upgrade women’s surgery. One result was specialized gynecologic OR nurse directors with telesurgery/telemedicine integrated into the suites. Digital platform cameras; smaller, clearer laparoscopes; and voice-activated lighting soon followed, as did better insufflators, image capturing, and other advances.
Today we rely on safer electrosurgery units (bipolar and tripolar) and “harmonic” energy.7 Tissue extractors enable us to remove large volumes of tissue quickly and safely. And all these developments have led to proven, enhanced outcomes for the patient.3
A promising future
The future for advanced operative laparoscopy is bright. As patients continue to press for minimally invasive procedures, the range of surgical options available to them will expand. To keep up, we will have little choice but to acquire expertise in minimally invasive applications.
Dr. Steven D. McCarus is a consultant to Ethicon Endo-Surgery and Gynecare.
Dr. Tamberly F. McCarus has no financial relationships relevant to this article.