Secondary gain often complicates diagnosis and therapy. Ask about current life events as well as any noteworthy happenings when the pain began. Consider the possibility of secondary gain or other psychological benefits of pain behaviors. For example, exaggerated response to pain and the reaction of significant others may be so reinforcing that pain behavior persists even after the painful stimulus has resolved. If you suspect this may be an issue, the patient should undergo psychological evaluation.
Pain may be psychologically debilitating. Evidence suggests that chronic pain itself, with or without organic pathology, produces debilitating psychological responses. Patients with such pain tend to feel depressed, helpless, and passive. They withdraw from social and sexual activity, and are preoccupied with pain and suffering.7 Personality testing of CPP patients without identified organic pathology shows characteristics similar to those of chronic pain patients with organic pathology. Specifically, on the Minnesota Multiphasic Personality Inventory, both these groups demonstrate a greater degree of anxiety, hypochondriasis, and hysteria than do control subjects.
Psychological response can affect organic processing of pain. A person’s psychological response to pain can influence how the nervous system transmits pain. Many neurotransmitters and neuromodulators can amplify or diminish pain impulses before pain signals reach the central nervous system. Anxiety and other psychological states may affect release and metabolism of these neurotransmitters, thus shaping perception of pain. Many forms of CPP, especially those with little or no pathology identified, may result primarily from disordered pain perception due to modulation of afferent impulses in the nervous system.
Excitatory modulators include substance P, glutamate, aspartate, calcitonin generelated peptide, and vasoactive intestinal peptide. Inhibitory neuromediators include endogenous opioid peptides, norepinephrine, serotonin (5-HT), and gamma-aminobutyric acid (GABA). Tricyclic antidepressants, other GABA-ergic agents, and selective serotonin reuptake inhibitors can increase inhibitory neuromediators, making them very useful in the management of CPP.
Referral to a multidisciplinary pain clinic is the most productive strategy for patients with noncyclic CPP and significant psychological issues.7 All patients with mental illness should be referred for psychological treatment.
A multidisciplinary facility typically includes a psychologist who also has expertise in sexual and marital counseling, an anesthesiologist, and—ideally—an acupuncturist, in addition to a gynecologist. Relaxation training, along with cognitive and behavioral therapies, can help train the patient to replace abnormal pain behavior and its secondary gain with effective, adaptive behavioral responses. Research has shown multidisciplinary management to be more effective than traditional episodic gynecologic management.
When a multidisciplinary pain clinic is unavailable, the gynecologist should involve other specialists by referral while coordinating the overall care of the patient.
What to do, what not to do when the cause is organic
Patients in whom an organic pathology is identified should be treated accordingly. Recent publications detail management strategies for endometriosis associated with CPP.1,5 For example, the algorithm in the Figure is based on a 2002 consensus statement.1
Procedures to avoid surgery in the absence of pathology. Without proof of organic pathology or a reasonable functional explanation for the pelvic pain, a thorough psychosomatic evaluation should be completed before a surgical corrective procedure is considered.
These procedures have not proven effective for noncyclic CPP without pathology:
- unilateral adnexectomy for unilateral pain
- total abdominal hysterectomy
- presacral neurectomy
- uterine suspension for generalized pelvic pain
- lysis of adhesions, which is usually nonproductive unless the site of laparoscopically visualized adhesions specifically coincides with the site of the local pain. Pelvic adhesions often recur following surgical lysis.
Another option: Acupuncture and nerve blocks. These strategies can provide prolonged pain relief in properly selected patients. Consultation with an anesthesiologist who is trained in chronic pain management can identify appropriate candidates. Acupuncture likely works by increasing spinal cord endorphins. Patients with trigger points usually respond well to injection of local anesthetics.
FIGURE Assessment, diagnosis, and treatment options for chronic pelvic pain and presumed endometriosis
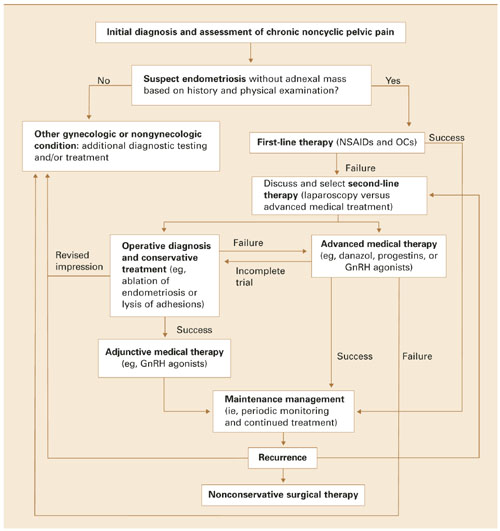
GnRH=gonadotropin-releasing hormone; NSAID=nonsteroidal antiinflammatory drug; OC=oral contraceptive Adapted from Fertil Steril; vol 78; Gambone JC, Mittman BS, Munro MG, Scialli AR, Winkel CA; Consensus statement for the management of chronic pelvic pain and endometriosis: proceedings of an expert-panel consensus process; 961-972; copyright 2002; with permission from American Society for Reproductive Medicine.
To prevent pain behaviors, schedule follow-up visits
In managing all patients with noncyclic CPP, take a supportive, sympathetic, and structured approach. This disorder is optimally treated in the context of an ongoing disease-management protocol rather than episodic therapy initiated because of a pain crisis.
Provide the patient with regular follow-up appointments; do not instruct her to call only when pain persists or recurs. The latter practice may create pain behaviors directed at obtaining sympathy and dramatic medical attention in certain patients.