Journal of Clinical Outcomes Management. 2015 September;22(9)
References
Promising results are emerging in the literature as researchers refocus their analysis on subgroups of depressed cardiac patients. In one large study of 442 depressed and 325 non-depressed patients, the number of depressive symptoms after an MI irrespective of the pre-MI depression status was associated with worse cardiac outcomes [47]. For every 1 additional depressive symptom reported 1 year post-MI, patients had a 15% increased risk for a new cardiac event in the next 2.5 years [47]. Another study demonstrated an improvement in depressive symptoms by 75.3% in in post-cardiac surgery patients with low ejection fraction (< 40%) after 8 weeks of nurse-guided CBT and worsening in depressive symptoms by 26.8% in usual care patients. More moderate findings were seen in the those with higher ejection fraction receiving the same CBT intervention for depression [45]. A treatment-resistant depression subgroup analyzed in a recent secondary analysis of the ENRICHD trial showed a twofold increase in mortality when compared to those in the non–treatment-resistant depression group [48]. Since treatment does not work for all patients with depression, including depressed post-MI patients, further evaluation with a focus on those who respond to treatment is needed.
Depression in Stroke
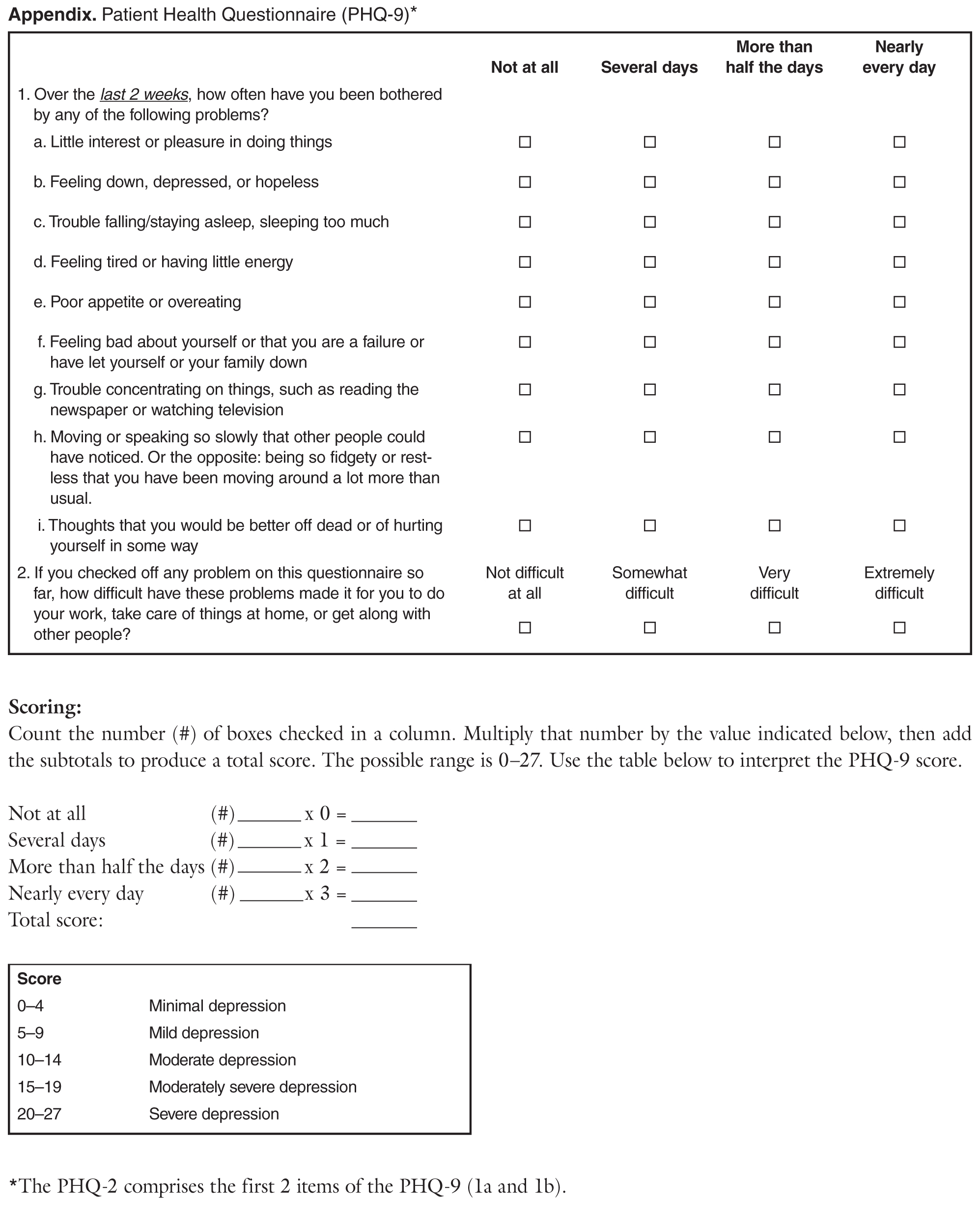
Depression has been reported to have a 39% to 53% incidence in stroke patients within 5 years of a stroke [25]. Compared to nondepressed stroke patients, depressed post-stroke patients experience an approximately 5 times increased risk for disability at 3 months post-stroke, along with a fourfold increase in anxiety, a 27% increase in mortality, and lower quality of life [49]. Regarding depression, stroke represents unique screening and treatment challenges. Apathy and depression can occur together or independently after stroke, with apathy having been reported at a higher rate than depression in post-stroke patients [50]. Since apathy is a disturbance of motivation presenting as no obvious emotions, indifference, and contentment with doing nothing, it is easily misinterpreted as depression [51] and occurs in more than half of those with depressed mood. A meta-analysis of 19 studies and 2221 stroke patients reported a 36.6% pooled rate of apathy, which was 3 times higher than the rate of depression [51]. In addition, up to 53% of post-stroke patients report pseudobulbar affect, defined as sudden and socially inappropriate laughing and crying, which adds to the complexity of screening for and diagnosing depression [52]. Given the challenges associated with post-stroke symptoms, screening post-stroke patients has been studied and reported as feasible using the Patient Health Questionnaire ( Appendix), which is recommended by the AHA for screening in cardiac patients [53].
Issues related to treatment of stroke patients parallel those of depressed patients with cardiac disease, as the effect on mortality and survival is unknown. Depression has been reported to go untreated in up to 67.9% of depressed post-stroke patients [54]. In addition, mismatches between antidepressant prescription and those with depression suggested that some patients without depression were being treated for depression while some patients with depression were not being treated [54].
Anxiety
Anxiety disorders create behavioral disturbances of fear and avoidance related to an individual’s propensity to overestimate dangers [21]. Though a number of anxiety disorders are described in the Diagnostic and Statistical Manual of Mental Disorders, 5th edition (DSM-5), anxiety as a general constellation of symptoms (afraid, inability to relax, worry about everyday problems, feelings of panic) is described in most of the literature related to CVD [55–57]. To a lesser extent, generalized anxiety disorder (GAD), defined as anxiety symptoms on more days than not and lasting more than 6 months [58,59] has also been studied. Because anxiety can be a component of depression, the 2 are often discussed together. Taken together, in the context of CHD, individuals with both anxiety and depression are at significantly greater risk for death (odds ratio 2.35, 95% confidence interval 1.23-4.47, P =0.01), compared with those without symptoms [60].