During the hospital stay in the postnatal period, women had their blood pressure monitored and antihypertensives were adjusted as needed. After discharge from the hospital, blood pressure was monitored by the family physician who also made decisions regarding antihypertensive management. All women had a follow-up visit in the hospital in the 6th postnatal week as per the postnatal clinic protocol.
Definitions
Hypertension was defined as BP ≥ 140/90 mm Hg. The hypertension disorders of pregnancy were defined as follows:
- Gestational hypertension: hypertension after 20 weeks gestation on two occasions 4 hours apart without meeting criteria for preeclampsia.
- Preeclampsia: hypertension after 20 weeks gestation on two occasions 4 hours apart with proteinuria (≥ 300 mg/24 hour) or, in the absence of proteinuria, new onset of any of the following: thrombocytopenia, renal insufficiency, impaired liver function, pulmonary edema, or cerebral or visual symptoms [1]. Severe preeclampsia was defined as preeclampsia with any of the following: systolic blood pressure > 160 mm Hg diastolic BP > 110 mm Hg or more on 2 occasions 4 hours apart, thrombocytopenia (platelet count < 100,00/mL), renal insufficiency, impaired liver function, pulmonary edema, or cerebral or visual symptoms. Preeclampsia without any of these features was considered nonsevere preeclampsia.
- Eclampsia: Women with hypertension with epigastric pain, headache, vomiting, and blurring of vision were diagnosed with imminent eclampsia and those with hypertension-related convulsions were diagnosed with eclampsia.
- Complications of preeclampsia included eclampsia, placental abruption, pulmonary edema, thrombocytopenia, HELLP syndrome, disseminated intravascular coagulation, multiorgan failure, severe intrauterine growth restriction, and fetal demise.
Main Outcome Measure
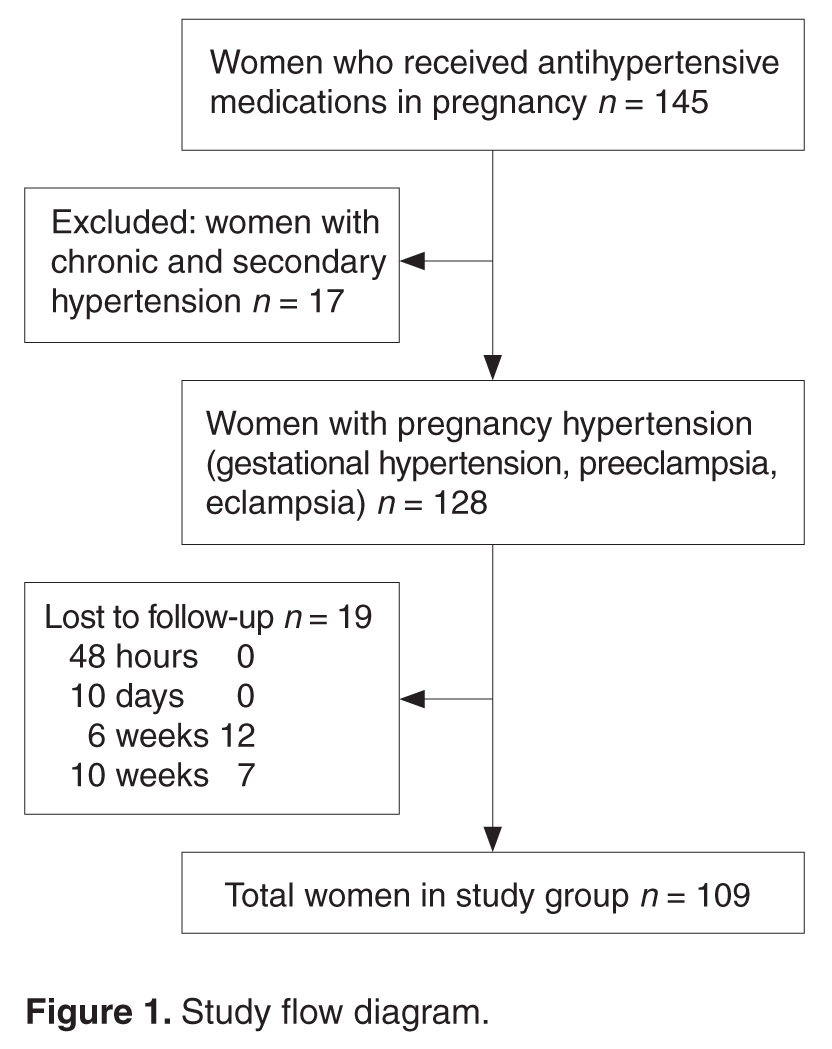
Time to reversion of hypertension was the main outcome measure. We defined the reversion date as the day that hypertension medications were stopped. This information was obtained via in-person questioning on the 2nd postpartum day and at the 6-week postnatal visit and via telephonic survey on the 10th postnatal day and at 10 weeks postdelivery. Women who missed the 6-week postnatal visit were also followed up by telephone.
Data Collection
Demographic details (age, parity, BMI) as well as information regarding gestational age at onset of hypertension, severity, highest systolic and diastolic blood pressure recordings, treatment received, complications related to hypertension, pregnancy termination and delivery was obtained from the medical charts and/or via telephonic follow-up.
Analysis
We used Pearson’s chi-square test to assess the association between recovery trends in blood pressure and the patient’s demographic profile and details of pregnancy hypertension. Statistical analysis was done using SPSS16.
Results
In our study, earlier the gestational age at onset of hypertension and earlier gestation at delivery was associated with slower recovery from hypertension ( Table 2 ). Time taken for recovery also was associated with age, BMI, severity of hypertension, associated complications, and the number of antihypertensive medications received (Table 2). Among women who received more than 3 antiphypertensives in pregnancy, nearly 50% continued to have hypertension beyond 6 weeks (Table 2).