Suicide Risk in Older Adults: The Role and Responsibility of Primary Care
Journal of Clinical Outcomes Management. 2017 April;24(4)
References
Second, safety planning is a brief intervention that may be beneficial in the primary care setting [67,68]. The goal of a safety plan is to create an individualized plan to remain safe during a suicidal crisis. Means safety discussion is the last of 6 steps in the safety plan [68]. The first 5 steps include identifying warning signs, using internal coping strategies, social connectedness as distraction, social support for the crisis, and professionals that can be used as resources. When patients can identify specific, individualized warning signs that occur prior to a crisis, they can then use strategies to cope and prevent the crisis from worsening. Coping strategies that are encouraged are first internal (ie, those that can be done without relying on anyone else), such as exercise or journaling. If those do not improve the patient’s mood, then he or she is encouraged to use people or social settings as a distraction (eg, people watching at the mall, calling an acquaintance to chat), and if he or she is still feeling bad, encouraged to get social support for the crisis (eg, calling a family member to discuss the crisis and get support). Finally, if all of these steps are not effective, the older adult is encouraged to reach out to professional supports, such as a mental health provider, the National Suicide Prevention Lifeline, or 911 (or go to an emergency room). Readers are encouraged to review Stanley and Brown’s articles for comprehensive details about safety planning as an intervention [67,68]. Additionally, an article with specific adaptations for safety planning with older adults is forthcoming [69].
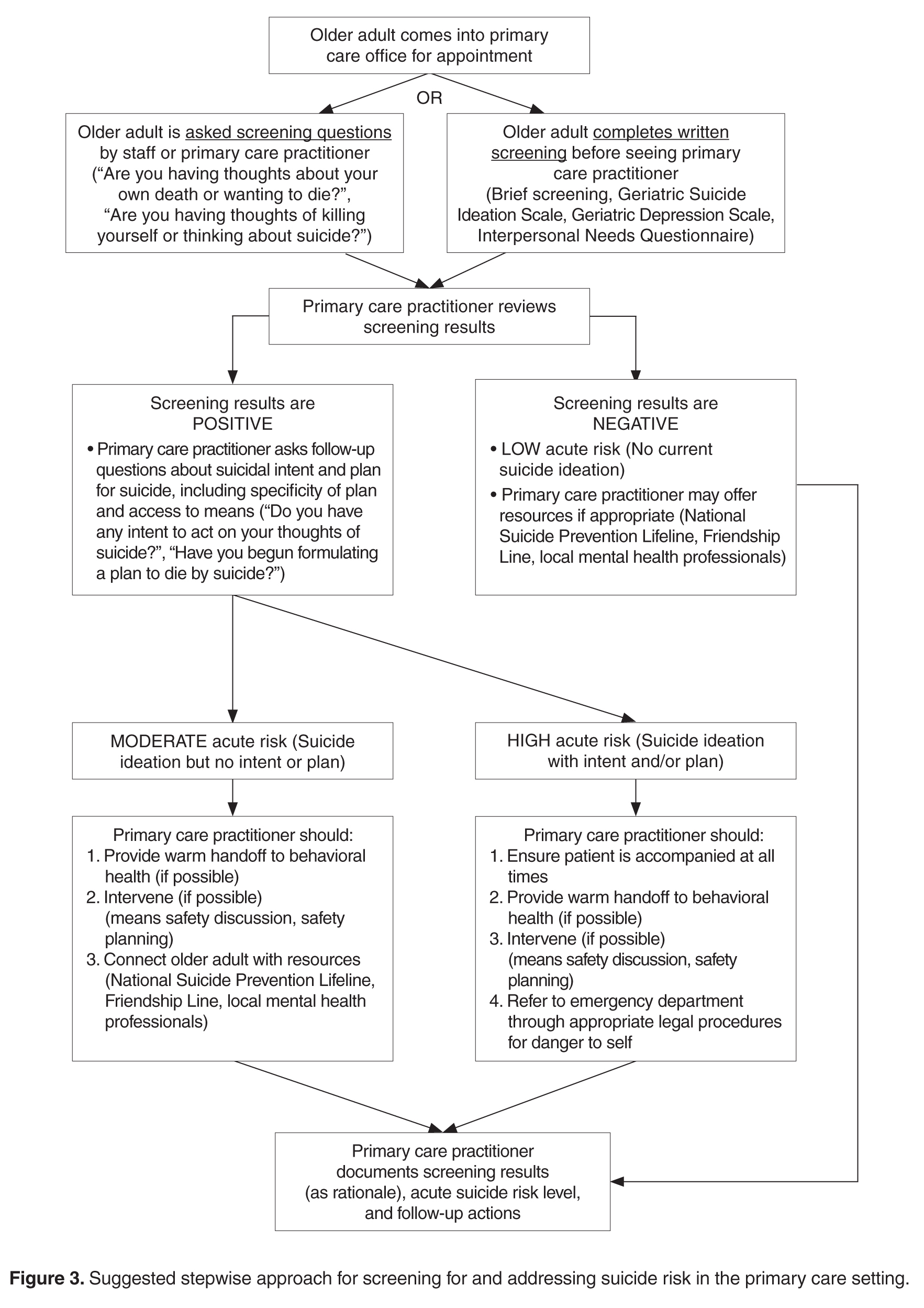
As noted above, collaborative care planning has been researched and shown to be effective for older adults in primary care. One trial introduced depression care managers and guidelines for depression care into 20 primary care practices [46]. Depression care managers offered psychotherapy and collaborative consultation with primary care physicians regarding interventions for depression. Patients in the intervention evidenced a faster reduction in suicide ideation than those receiving usual care and, among those who reported suicide ideation at baseline, suicide ideation resolved more quickly in patients who received the intervention [46]. These results were sustained over 2 years; significantly fewer patients with major depression who received the intervention reported suicide ideation at 24 month follow-up than patients who had received usual care [47]. In a separate study that also introduced depression care managers to primary care practices, results suggested that fewer older adults who received the intervention reported suicide ideation at all time points, up to 24 months later [48]. Depression care managers in this study provided psychotherapy and offered psychoeducation about depression treatment options [48]. Additionally, though there is not specific evidence for the feasibility of safety planning in primary care at this time, research has found it to be feasible and acceptable in an emergency department setting [70]. Emergency departments, similar to primary care settings, place significant demands on physicians’ time. Collectively, these results suggest that behavioral interventions can be successfully implemented, even in busy primary care settings. See Figure 3