Deprecated function: Return type of DatabaseStatementBase::execute($args = [], $options = []) should either be compatible with PDOStatement::execute(?array $params = null): bool, or the #[\ReturnTypeWillChange] attribute should be used to temporarily suppress the notice in require_once() (line 2246 of /var/www/webmd/apps/mdedge/htdocs/includes/database/database.inc).
Deprecated function: Return type of DatabaseStatementEmpty::current() should either be compatible with Iterator::current(): mixed, or the #[\ReturnTypeWillChange] attribute should be used to temporarily suppress the notice in require_once() (line 2348 of /var/www/webmd/apps/mdedge/htdocs/includes/database/database.inc).
Deprecated function: Return type of DatabaseStatementEmpty::next() should either be compatible with Iterator::next(): void, or the #[\ReturnTypeWillChange] attribute should be used to temporarily suppress the notice in require_once() (line 2348 of /var/www/webmd/apps/mdedge/htdocs/includes/database/database.inc).
Deprecated function: Return type of DatabaseStatementEmpty::key() should either be compatible with Iterator::key(): mixed, or the #[\ReturnTypeWillChange] attribute should be used to temporarily suppress the notice in require_once() (line 2348 of /var/www/webmd/apps/mdedge/htdocs/includes/database/database.inc).
Deprecated function: Return type of DatabaseStatementEmpty::valid() should either be compatible with Iterator::valid(): bool, or the #[\ReturnTypeWillChange] attribute should be used to temporarily suppress the notice in require_once() (line 2348 of /var/www/webmd/apps/mdedge/htdocs/includes/database/database.inc).
Deprecated function: Return type of DatabaseStatementEmpty::rewind() should either be compatible with Iterator::rewind(): void, or the #[\ReturnTypeWillChange] attribute should be used to temporarily suppress the notice in require_once() (line 2348 of /var/www/webmd/apps/mdedge/htdocs/includes/database/database.inc).
Clinical Review
Chronic Obstructive Pulmonary Disease: Epidemiology, Clinical Presentation, and Evaluation
Journal of Clinical Outcomes Management. 2017 April;24(4)
References
In the Lung Health Study, which evaluated patients with mild COPD, more women than men demonstrated increased airway responsiveness, although this difference was thought to be related to airway caliber rather than gender [42]. Adult women are more likely to both develop and die of asthma than are men [43–45]. In NHANES III, whereas women reported more physician-diagnosed COPD and asthma than men, men and women had similar rates of decreased lung function, and a similar proportion of both men and women with low lung function had undiagnosed lung disease [3]. The current evidence is inadequate to determine whether women who smoke are more likely to develop COPD or have more severe COPD than men, although this question is being studied by various groups.
Risk Factors and Etiology
Smoking is the dominant risk factor for the development and progression of COPD; however, not all smokers develop COPD, and COPD does occur in persons who have never smoked [1], suggesting that other factors are important in the etiology of COPD. Alpha1-antitrypsin deficiency is an important cause of COPD in a very small percentage of cases [46]. Other undefined genetic factors certainly play an important role in COPD development [38]. The role of infections in both the development and progression of COPD is receiving increased attention, including the role of adenoviral infections in emphysema [47–49].
Occupational and environmental exposures to various pollutants (eg, particulate matter, agricultural dusts) are also important factors in the development of COPD [50,51]. Exposure to indoor air pollutants such as smoke from solid biomass fuels is a major risk factor for COPD especially among women and children in low- and middle-income countries [52,53]. Occupational exposure to fumes and dusts remains an important cause for COPD globally [53,54]. Exposure to outdoor air pollution is associated with a risk of development of COPD as well as exacerbation of the existing disease [53,55].
Clinical Presentation
COPD is heterogeneous in its presentation. Based on data from NHANES III, 44% of patients with severe airflow limitation (FEV 1 < 50% of predicted) may not report symptoms [3]. Among patients with severe airflow limitation who do report symptoms, the symptoms reported most frequently include wheezing (64%) and shortness of breath (65%).
In recent years, COPD has been increasingly recognized as a systemic illness, with effects on nutritional status, muscle wasting, and depression [56–58]. A large proportion of patients probably have components of chronic bronchitis, asthma, and emphysema occurring together. Although some of this overlap may be related to misdiagnosis, some of it may be a measure of the presence of airflow limitation reversibility, as described above. Better defining individuals in these groups may ultimately help tailor better interventions.
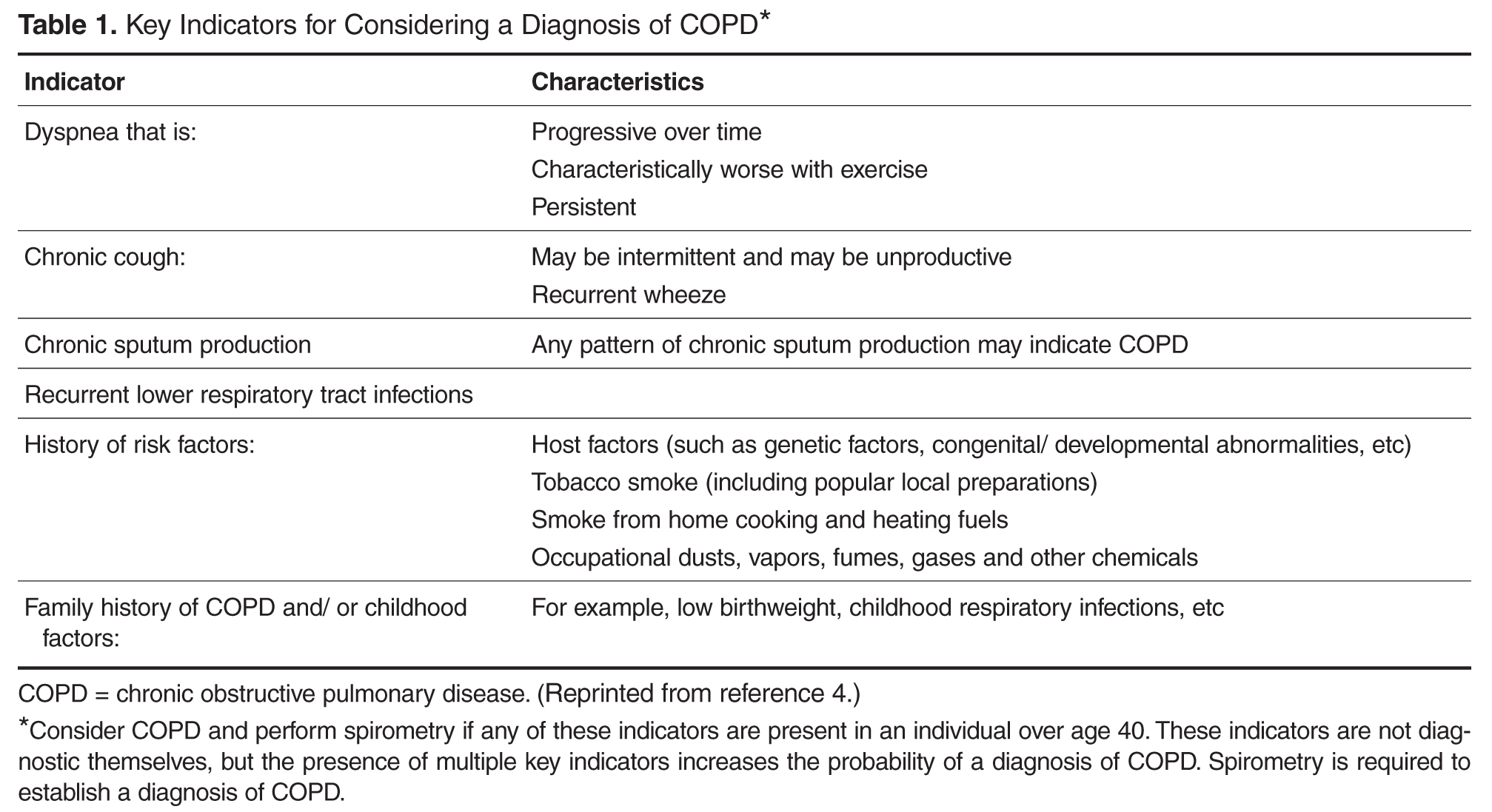
Key indicators for considering a diagnosis of COPD are listed in Table 1 . These indicators are either the presence of symptoms (chronic cough, chronic sputum production, or dyspnea) or a history of smoking or exposure to occupational dusts or chemicals. Spirometry with an evaluation of bronchodilator response is then needed to establish a diagnosis of COPD. Based on prior data, at least 67% of the adult US population would have at least 1 of these indicators present [3]. The proportion of the US population that has had pulmonary function testing is unknown but is thought to be very low. Abnormal findings on the office-based spirometry should be followed up with diagnostic-quality spirometry, including the determination of reversibility.
Some of the barriers to COPD diagnosis and subsequent treatment often include insufficient knowledge and awareness about COPD especially among primary care physicians, misdiagnosis of COPD as other respiratory diseases such asthma, as well as patient-related barriers involving lack of awareness of early symptoms of COPD and considering them to be related to aging or smoking [59].