Mary J. Aigner, PhD, RN, FNP-BC; and Pawan Sikka, MD
Dr. Sikka is the chief of Pulmonary, Critical Care, and Sleep Medicine, at the Central Texas Veterans Health Care System in Temple, Texas. Dr. Aigner was an advanced practice registered nurse practitioner in Pulmonary and Sleep Medicine at the Central Texas Veterans Health Care System at the time the article was written and is now retired.
It is recommended that the surgeon and anesthesiologist ask about a diagnosis of OSA or sleep apnea symptoms during the preanesthesia assessment for any surgery. The provider performing the preoperative physical examination should pay attention to the circumference of the neck, chin-throat length, Mallampati classification, mandible position, and BMI. Any findings that suggest undiagnosed OSA should prompt further evaluation before any elective surgery.
Those who are at risk of OSA anesthesia-related complications should be offered regional anesthesia if possible. It is undesirable to premedicate with sedatives or opioids for this population. The sniffing position during surgery has been found to reduce the collapsibility of the airway and improve its dimensions. All patients who use CPAP therapy at home should have this therapy available for use in the recovery room with the lateral position preferred.17
Outpatient surgery using sedation and local anesthetics can also be a higher risk for patients with OSA. The unprotected, potentially problematic airway is still a serious concern. Patients requiring short procedures may do well with titrated sedation if well positioned and appropriately selected for this before the procedure. Clinicians must be prepared to handle any complications that occur. One complication that occurs commonly in obese patients related to a smaller functional residual capacity is rapid oxygen desaturation.17
A Chinese study evaluated complications in patients who had received tongue base reduction through RFA. Complications, both intraoperative and postoperative, included hematoma of the tongue base, bleeding, altered taste, an abscess at the base of the tongue, speech dysfunction, numbness, and deviation of the tongue extension movement. One cardiac death occurred 37 hours following surgery related to swelling of the tongue base and pain, which aggravated sleep apnea and nocturnal hypoxemia and induced a fatal arrhythmia.15
The Future of OSA Treatments
Research is underway to evaluate the effectiveness of an implanted system to stimulate the hypoglossal nerve with the intent of activating the upper airway musculature. A small study of 8 patients found improvement in the degree of upper airway collapsibility and the severity of OSA. Continued research on the device is focusing on the parameters for the nerve stimulation. The criteria for patient selection are also being established.20
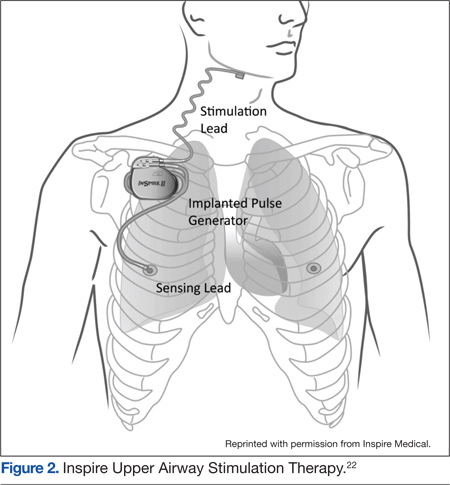
Another study of hypoglossal nerve stimulation (HNS) evaluated 21 patients who were unable to tolerate CPAP therapy. The researchers found significant improvement in AHI (43.1 + 17.5 to 19.5 + 16.7); Functional Outcomes of Sleep Questionnaire (14.4 + 2.0 to 16.7 + 2.2); ESS (12.1 + 4.7 to 8.1 + 4.4); Beck Depression Inventory (15.8 + 9.0 to 9.7 + 7.6); and the Calgary Sleep Apnea Quality of Life Index (3.2 + 1.0 to 4.9 to 4.9 + 1.3). The researchers concluded HNS decreased OSA-related symptoms and the severity of OSA.21 At least one of these devices, the Inspire device, has been approved for use in Europe (Figure 2).22 In addition, the FDA has approve the Inspire Upper Airway Stimulation therapy for use in a subset of patients with moderate to severe OSA who are unable to use CPAP.23
A recent study investigated the effect of HNS on the severity of OSA among patients who had moderate to severe OSA and had not had a response to CPAP therapy. The HNS was associated with significant improvement in reducing the frequency of respiratory events. The median AHI at 12 months decreased from 29.3 events per hour to 9.0 events per hour (P < .001), and the number of times per hour of sleep that the blood oxygen level dropped by ≥ 4% from the baseline (oxygen desaturation index score) decreased from 25.4 to 7.4 events per hour (P < .001).24
Another area being studied is the development of a device to advance the tongue. Forty-two patients had mandibular bone anchors inserted with a flexible tether connected to a surgically inserted anchor in the posterior tongue. Unfortunately, 31% of the participants developed tissue anchor barb fractures that were asymptomatic and detected through radiography. At this time, the failure rate does not warrant clinical use. However, some patients showed significant improvement in multiple measures for sleep apnea, and more research is ongoing with the device.25
Similarly, a surgically inserted tongue pin that connects to an oral device during sleep has been studied. This pin prevents the tongue from moving back and obstructing the upper airway. Polysomnographies were performed both before and after and showed an increased rate of apnea in the 10 subjects. Visualization with magnetic resonance imaging showed that the upper airway was not kept open by this fixation device. Additional research with a modified design for the device is recommended.26