By Matthew McAdams, MA; Lynne Cannavo, RN, MSN; and Jay D. Orlander, MD, MPH
Mr. McAdams is a third-year medical student at the Boston University School of Medicine; Ms. Cannavo is the director of quality management and Dr. Orlander is associate chief of the medical service, both at the VA Boston Healthcare System; Dr. Orlander is also a Professor of Medicine at the Boston University School of Medicine and the Evans Department of Medicine, Section of General Internal Medicine, both in Boston, all in Massachusetts.
This article reports the initial experience with the implementation of an e-Consult system for PCPs and medical subspecialists in a large VA health care system. Primary care providers were generally satisfied with the e-Consult system and reported that the system yielded tangible benefits to patients, such as quicker specialty input and avoidance of FTF visits and travel. Specialists were somewhat less satisfied than were their primary care colleagues; nevertheless, specialists perceived similar benefits for patients. Despite the general satisfaction among PCPs, > 1 in 4 specialists expressed dissatisfaction with the system.
Satisfaction with e-Consults may be influenced by the typology of the specialty itself. Some specialties (eg, hematology) rely more heavily on laboratory tests, compared with specialties such as cardiology, gastroenterology, or pulmonary whose subtleties of history and physical examination (H&P), along with review of imaging data, are more commonly required for clinical decision making.2 Hence, the EHR may allow some specialties to provide e-Consults with greater facility. For example, because the EHR enables clinicians to trend the results of years of complete blood counts with a few simple keystrokes, a hematologist may have more confidence in making a clinical assessment without seeing the patient based on historical information in the EHR.
Anecdotal evidence from specialists suggests discomfort when clinical input is based on H&P findings of others. While the sample size was small, this reasoning could explain the differences in satisfaction among specialties: Satisfied specialists may be taking slightly less time to complete their e-Consults, but they were less likely to view the e-Consult as new work and less likely to convert to a FTF consultation.
Store-and-forward telemedicine cannot completely replace FTF visits, but rather supplement them. If e-Consults obviate patient travel and copays while stimulating more timely completion of the consultation, the benefits of cost savings and improved specialty access by veterans merit further attention. When an e-Consult did not avoid a FTF consultation, the majority of clinicians perceived that the e-Consult allowed the PCP to initiate diagnostic testing or alterations in treatment prior to the eventual FTF consultation with the specialist. This finding could be considered as a proxy for increased coordination of care between primary care and specialty providers in anticipation of a FTF visit.
During the study period, workload capture for e-Consults was administratively fixed at the level of a brief consultation, regardless of the effort expended. Validation of the current finding regarding time spent completing consults has resulted in a change. On January 10, 2014, VA Central Office updated its policy to allow 3 levels of workload credit for e-Consults based on time: up to 15 minutes, 16 to 30 minutes, and > 30 minutes.
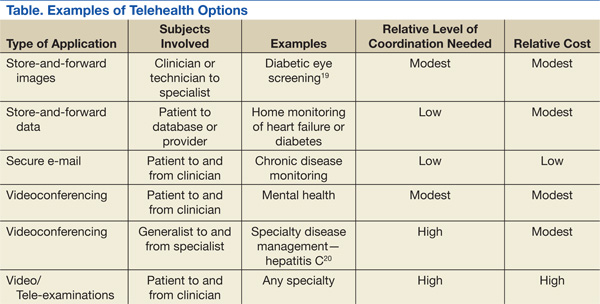
E-consults are just one example of innovations that broadly fall under the rubric of telehealth initiatives being deployed across VA health care facilities. Other examples of SAFT include pictures collected by technicians and sent to specialists for review to screen for diabetic retinopathy, a practice done within VA for many years.19 Clinical video telehealth provides real-time videoconferencing between patient and specialist and can obviate the need for long-distance patient travel. Initially used only for interviews, newer equipment amplifies sound and enhances optical imaging to allow thorough physical examinations when trained personnel are handling the equipment.
Each technology has its challenges for implementation, which vary in degree of coordination and cost. Overall, the application of new technologies and repurposing existing ones may be limited by creativity alone in the efforts to improve access and quality of the care provided to veterans. The Table highlights telehealth uses being deployed by VA.
Conclusion
Electronic consults have been well received by PCPs and most specialists in the VABHS, seeming to meet the goal of using telehealth to improve veterans’ access to specialty care and coordination of care between PCPs and specialists. While not examined in this initial report, e-Consults may lead to reduced costs, and this possibility should be further explored.
Despite concerns expressed by some specialists, most believed that e-Consults improved the quality of care their patients received. Future work needs to validate these findings, examine patient perspectives, delve more deeply into ways to improve and bring more value to the process, and address the specialty effort in relation to workload awarded.
Acknowledgements The authors would like to thank Yisraela Elstein and Pauline Benedetti for their assistance in tracking workload data and Steven Simon for his detailed review of the manuscript. Funding for this work was supported by the Department of Veterans Affairs Specialty Care Transformation Initiative for the 21st Century—T21 innovation grant for telehealth initiatives.