Kelly Colas, DO, PhDa; Kavita Vyas, MDb,c; Dipa K. Sheth, MDa,c,d Correspondence: Kelly Colas (kcolas@uw.edu)
aDepartment of Allergy and Immunology, University of Washington, Seattle bDepartment of Pulmonary and Critical Care, Washington DC Veterans Affairs Medical Center cGeorge Washington University, Washington, DC dUniformed Services University of the Health Sciences, Bethesda, Maryland
Author disclosures
The authors report no actual or potential conflicts of interest or outside sources of funding with regard to this article.
Disclaimer
The opinions expressed herein are those of the authors and do not necessarily reflect those of Federal Practitioner, Frontline Medical Communications Inc., the US Government, or any of its agencies. This article may discuss unlabeled or investigational use of certain drugs. Please review the complete prescribing information for specific drugs or drug combinations—including indications, contraindications, warnings, and adverse effects—before administering pharmacologic therapy to patients.
Ethics and consent
The intention of this project was to examine the implementation of a program for the improvement of patient care. As this project is qualitative improvement, it did not qualify for institutional review board approval.
If patients continued to experience asthma exacerbations after the initiation of a biologic, a change in agent was considered after 4 to 6 months. Additionally, a complete blood count, respiratory allergy panel, and pulmonary function tests (PFTs) were completed.
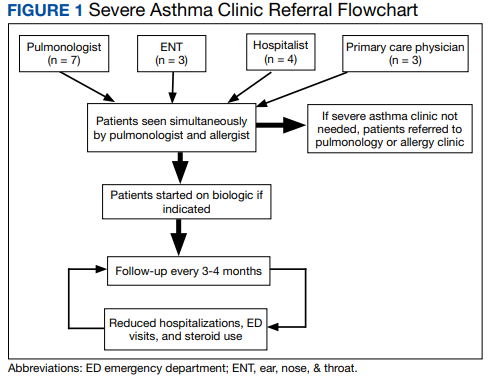
If a patient experienced an allergic reaction, the biologic agent was stopped. All patients had access to secure messaging to both the allergist and pulmonologist at this clinic. Figure 1 illustrates the general flow of our severe asthma clinic.
Clinic Patients
Preliminary data were obtained from a retrospective chart review of 15 patients enrolled in the severe asthma clinic over 30 months. The inclusion criteria for chart review consisted of patients aged > 18 years receiving a biologic agent for > 3 months for the treatment of severe asthma. The outcomes examined included steroid use, emergency department (ED) visits, hospitalizations, FEV1, and ICU stays.
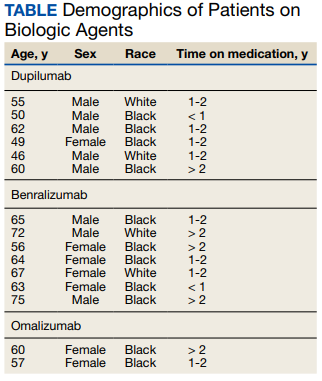
Seven patients used benralizumab, 6 used dupilumab, and 2 used omalizumab (Table).
Of the patients examined, 8 had been on a biologic agent for 1 to 2 years while a smaller number of patients had been taking a biologic agent for less than a year (n = 2) or > 2 years (n = 5). Seven patients were referred to the specialty asthma clinic by a VA pulmonologist, 4 were referred by a hospitalist, 3 by an otolaryngologist, and 3 by their primary care physician.