Maren Scheuner is a Professor in Medicine and Pediatrics at the University of California, San Francisco School of Medicine and the Director of the Clinical Genetics Program, San Francisco US Department of Veteran Affairs (VA) Health Care System. Kenute Myrie is a Portfolio Manager for Oncology and Lead for Precision Oncology, Clinical Science Research and Development Service, VA Office of Research and Development Jane Peredo is a Genetic Counselor at the Greater Los Angeles VA Healthcare System in California. Lori Hoffman-Hogg is Program Manager for the Veterans Health Administration (VHA), National Center for Health Promotion and Disease Prevention in Durham, North Carolina, and National Oncology Clinical Advisor for the Office of Nurses Services in Washington, DC. Margaret Lundquist is a Nurse Practitioner and Douglas Ball is a Staff Physician with the Genomic Medicine Service, VHA Central Office. Stephanie Guerra is an American Association for the Advancement of Science (AAAS) and Science and Technology Policy Fellow, VA Office of Research and Development.
Author disclosures The authors report no actual or potential conflicts of interest with regard to this article.
Disclaimer The opinions expressed herein are those of the authors and do not necessarily reflect those of Federal Practitioner, Frontline Medical Communications Inc., the US Government, or any of its agencies.
Objectives: The advent of germline testing as a standard-of-care practice for certain tumor types and patients presents unique opportunities and challenges for the field of precision oncology. This article describes strategies to address workforce capacity, organizational structure, and genetics education needs within the US Department of Veterans Affairs (VA) with the expectation that these approaches may be applicable to other health care systems.
Observations: Germline information can have health, reproductive, and psychosocial implications for veterans and their family members, which can pose challenges when delivering germline information in the setting of cancer care. Additional challenges include the complexity inherent in the interpretation of germline information, the national shortage of genetics professionals, limited awareness and knowledge about genetic principles among many clinicians, and organizational barriers, such as the inability to order genetic tests and receive results in the electronic health record. These challenges demand thoughtful implementation planning at the health care system level to develop sustainable strategies for the delivery of high-quality genetic services in precision oncology practice.
Conclusions: The VA is uniquely positioned to address the integration of germline genetic testing into precision oncology practice due to its outsized role in treating veterans with cancer, training the health care workforce, and developing, testing, and implementing innovative models of clinical care.
The US Department of Veterans Affairs (VA) oversees the largest integrated health care system in the nation, administering care to 9 million veterans annually throughout its distributed network of 1,255 medical centers and outpatient facilities. Every year, about 50,000 veterans are diagnosed with and treated for cancer in the VA, representing about 3% of all cancer cases in the US.1 After skin cancer, prostate, colon, and lung cancers are the most common among veterans.1 One way that VA has sought to improve the care of its large cancer patient population is through the adoption of precision oncology, an ever-evolving practice of analyzing an individual patient’s cancer to inform clinical decision making. Most often, the analysis includes conducting genetic testing of the tumor itself. Here, we describe the opportunities and challenges of integrating germline genetics into precision oncology practice.
The Intersection of Precision Oncology and Germline Genetics
Precision oncology typically refers to genetic testing of tumor DNA to identify genetic variants with potential diagnostic, prognostic, or predictive therapeutic implications. It is enabled by a growing body of knowledge that identifies key drivers of cancer development, coupled with advances in tumor analysis by next-generation sequencing and other technologies and by the availability of new and repurposed therapeutic agents.2 Precision oncology has transformed cancer care by targeting both common and rare malignancies with specific therapies that improve clinical outcomes in patients.3
Testing of tumor DNA can reveal both somatic (acquired) and germline (inherited) gene variants. Precision oncology testing strategies can include tumor-only testing with or without subtraction of suspected germline variants, or paired tumor-normal testing with explicit analysis and reporting of genes associated with germline predisposition.2 With tumor-only testing, the germline status of variants may be inferred and follow-up germline testing in normal tissue such as blood or saliva can be considered. Paired tumor-normal testing provides distinct advantages over tumor-only testing, including improvement of the mutation detection rate in tumors and streamlining interpretation of results for both the tumor and germline tests.
Regardless of the strategy used, tumor testing has the potential to uncover clinically relevant germline variation associated with heritable cancer susceptibility and other conditions, as well as carrier status for autosomal recessive disorders (eAppendix
). For example, in the VA, there is widespread use of a 309-gene tumor-testing panel. When we searched the Online Mendelian Inheritance in Man database (www.omim.org) for these 309 genes, we found 156 (50.5%) were associated with 230 hereditary disorders that have potential clinical relevance for adults. (We excluded disorders with developmental delay, intellectual disability, and/or multiple congenital anomalies.) Of the 230 hereditary disorders, 86 (37.4%) are associated with inherited cancer predisposition with the remainder associated with neurologic, cardiovascular, immunodeficiency, metabolic, overgrowth syndromes, and other disorders. Almost 70% of the 230 disorders are due to autosomal dominant inheritance, and 11 (5%) are due to somatic mosaicism (eg, McCune Albright syndrome, Sturge-Weber syndrome, and Proteus syndrome). Fifty-eight (25%) are due to autosomal or X-linked recessive inheritance with reproductive implications for veterans or their family members (eg, Fanconi anemia, constitutional mismatch repair deficiency, juvenile Parkinson disease type 2, retinitis pigmentosa 38, and spastic paraplegia 45).
Germline genetic information, independent of somatic variation, can influence the choice of targeted cancer therapies. For example, Mandelker and colleagues identified germline variants that would impact the treatment of 38 (3.7%) of 1,040 patients with cancer.4 Individuals with a germline pathogenic variant in a DNA repair gene (eg, BRCA1, BRCA2, ATM, CHEK2) are candidates for platinum chemotherapy and poly-(adenosine diphosphate-ribose) polymerase (PARP) inhibitors that target the inability of a tumor to repair double-stranded DNA breaks.5,6 Individuals with a germline pathogenic variant in the MSH2, MLH1, MSH6, PMS2 or EPCAM genes (ie, Lynch syndrome) have tumors that are deficient in mismatch repair, and these tumors are responsive to inhibitors of the programmed death 1 (PD1) pathway.7,8
In addition to changing treatment decisions, identifying pathogenic germline variants can have health, reproductive, and psychosocial implications for the patient and the patient’s family members.9,10 A pathogenic germline variant can imply disease risk for both the patient and his or her relatives. In these cases, it is important to ascertain family history, understand the mode of inheritance, identify at-risk relatives, review the associated phenotype, and discuss management and prevention options for the patient and for family members. For example, a germline pathogenic variant in the BRCA2 gene is associated with increased risk for breast, ovarian, pancreatic, gastric, bile duct, and laryngeal cancer, and melanoma.11 Knowledge of these increased cancer risks could inform cancer prevention and early detection options, such as more frequent and intensive surveillance starting at younger ages compared with that of average-risk individuals, use of chemoprevention treatments, and for those at highest risk, risk-reducing surgical procedures. Therefore, reporting germline test results requires the clinician to take on additional responsibilities beyond those required when reporting only somatic variants.
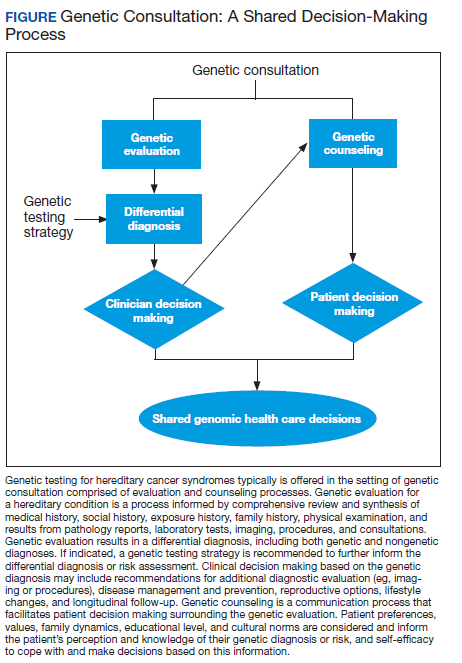
Because of the complexities inherent in germline genetic testing, it traditionally is offered in the context of a genetic consultation, comprised of genetic evaluation and genetic counseling (Figure). Clinical geneticists are physicians certified by the American Board of Medical Genetics and Genomics (a member board of the American Board of Medical Specialties) who received special training in the diagnosis and management of medical genetic conditions; they are trained to perform all aspects of a genetic consultation across the clinical spectrum and lifespan of a patient.12 In contrast, genetic counselors have a master’s degree in genetic counseling, a communication process that facilitates patient decision making surrounding the genetic evaluation.13 Most work as members of a team to ensure provision of comprehensive clinical genetic services. Genetic counselors are licensed in most states, and licensure in some states sanctions the ordering of genetic tests by genetic counselors. Genetics nurses are licensed professional nurses with special education and training in genetics who function in diverse roles in industry, education, research, and clinical care.14 Genetics nurses in clinical care perform risk assessment based on personal and family history, recognize and identify genetic conditions and predispositions, and discuss the implications of this with patients and their families. Advanced practice nurses (APRNs) have additional training that allows for diagnosis, interpretation of results, and surveillance and management recommendations.15