Tanner Caverly, Sarah Krein, and Laura Damschroder are Research Investigators; Claire Robinson and Jane Forman are Qualitative Analysts; and Sarah Skurla is a Research Associate; all at the VA Ann Arbor Health Care System, Center for Clinical Management Research, Health Services Research and Development in Michigan. Martha Quinn is a Research Specialist at the School of Public Health; Tanner Caverly is an Assistant Professor in the Medical School; and Sarah Krein is an Adjunct Research Professor in the School of Nursing; all at the University of Michigan in Ann Arbor. Correspondence: Tanner Caverly (tcaverly@med.umich.edu
Participants were asked to fill out a survey on arrival in the morning and were assigned to 1 of 3 tables or small groups. Each table had a facilitator who had extensive experience in qualitative data collection methods and guided the dialogue using a scripted protocol that they helped develop and refine. The facilitation materials drew from and used previously published studies.22,23 Each facilitator audio recorded the sessions and took notes. Three experts presented during plenary education sessions. Presentations were designed to provide balanced factual information and included a veteran’s perspective. One presenter was a clinician on the project team, another was a local clinical leader responsible for making decisions about what services to provide via civilian care (buy) vs enhancing the local VHA health system’s ability to provide those services (build), and the third presenter was a veteran who was on the project team.
Education Session 1
The first plenary education session with expert presentations was conducted after each table completed an icebreaker exercise. The project team physician provided a brief history and description of the Choice Act to reinforce educational materials sent to participants prior to the session. The health system clinical leader described his decision process and principles and highlighted constraints placed on him by the Choice Act that were in place at the time of the DD session. He also described existing local and national programs to provide civilian care (eg, local fee-basis non-VHA care programs) and how these programs sought to achieve goals similar to the Choice Act. The veteran presenter focused on the importance of session participants providing candid insight and observations and emphasized that this session was a significant opportunity to “have their voices heard.”
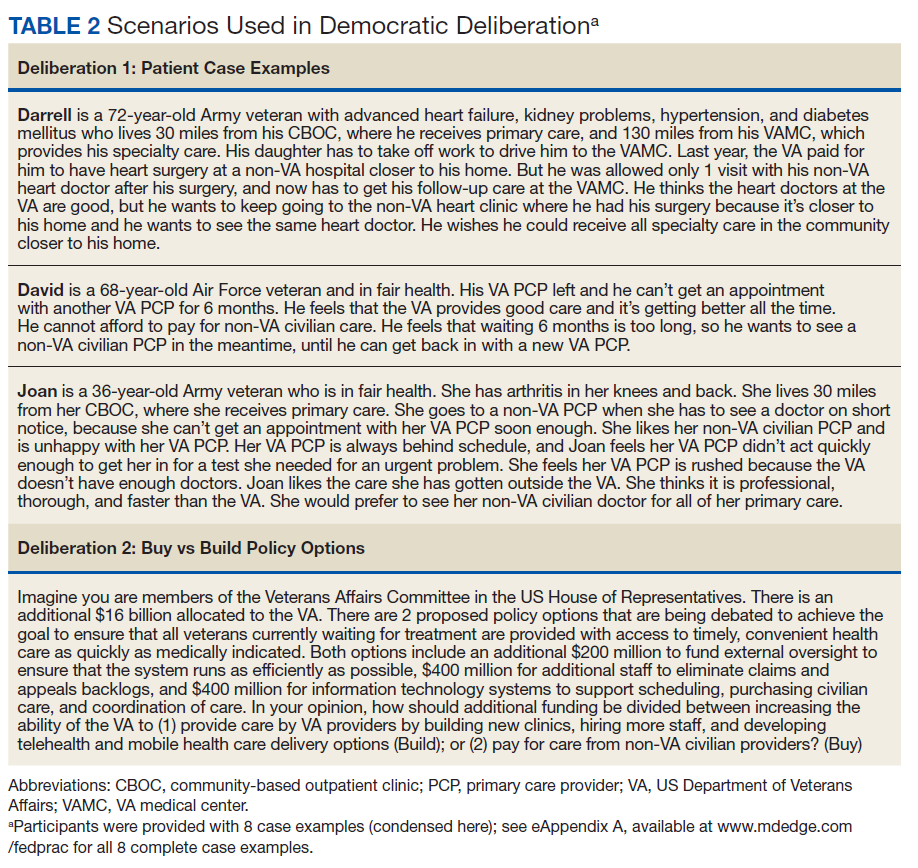
Deliberation 1: What criteria should be used to prioritize patients for receiving civilian care paid for by the VHA? To elicit preferences on the central question of this deliberation, participants were presented with 8 real-world cases that were based on interviews conducted with Choice Act-eligible veterans (Table 2 and eAppendices A
). Participants were first instructed to read through and discuss the cases as a group, then come to agreement on prioritizing how the patients in the case scenarios should receive civilian care. Agreement was defined as having complete consensus or consensus by the majority, in which case, the facilitator noted the number who agreed and disagreed within each group. The facilitators documented the criteria each group considered as they prioritized the cases, along with the group’s reasoning behind their choices.
Education Session 2
In the second plenary session, the project team physician provided information about health care access issues, both inside and outside of the VHA, particularly between urban and rural areas. He also discussed factors related to the insufficient capacity to meet growing demand that contributed to the VHA wait-time crisis. The veteran presenter shared reflections on health care access from a veteran’s perspective.
Deliberation 2: How should additional funding be divided between increasing the ability of the VHA to (1) provide care by VHA HCPs; and (2) pay for care from non-VHA civilian HCPs? Participants were presented the patient examples and Choice Act funding scenarios (the buy policy option) and contrasted that with a build policy option. Participants were explicitly encouraged to shift their perspectives from thinking about individual cases to considering policy-level decisions and the broader social good (Table 2).