Symptoms and Examination
Osteoarthritis encompasses a wide spectrum of common conditions with similar pathophysiology. Most of these conditions share similar historic features, including pain during or after use and stiffness after prolonged periods of inactivity. Other common symptoms include swelling, joint locking or “cracking,” instability, and joint fatigue. Patients may perceive OA discomfort in different ways. Whereas one patient with knee OA may describe a sharp, gnawing pain, another may experience painless swelling and instability. Although OA is mainly considered a localized disease, patients may present with multiple areas of pain, suggesting a more generalized pattern. Patients with OA may have short periods of morning stiffness and “gelling,” but prolonged stiffness suggests the presence of inflammatory arthritis.
Examination of the osteoarthritic joint is performed with thorough palpation and range of motion testing. Evidence of joint swelling may be present near the joint line with pain on palpation. Palpable crepitus is commonly noted with restricted range of motion, usually inducing pain at the maximal range. Osteophytes or chondrophytes at the joint line may be tender and are commonly mistaken for joint swelling. In the hands, bony hypertrophy of the PIP and DIP joints may be noted (Bouchard’s and Heberden’s nodes, respectively). Pain at the base of the thumb is a common complaint in patients with OA of the CMC joint.
Most cases of OA can be diagnosed by taking a history and a physical examination without further investigation; however, plain radiographs are frequently obtained to confirm the diagnosis. Joint inflammation, when present, is usually mild. Occasionally, patients may present with evidence of warmth, effusion, and severe pain with restriction of motion. Patients with these symptoms should undergo prompt arthrocentesis to rule out infection, crystal-associated arthritis, hemarthrosis, or other inflammatory causes.
Radiographic Features
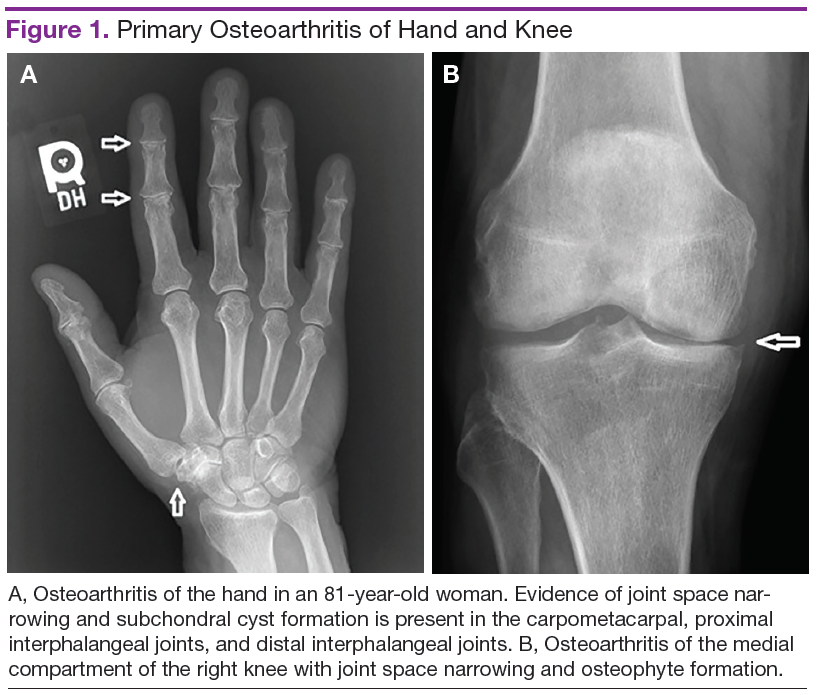
Plain radiographs are extremely helpful in denoting the extent of OA in a particular joint. Radiographic features of OA include narrowing of the joint space, osteophyte formation, and subchondral bone abnormalities. Narrowing of the joint space and alignment abnormalities occur due to loss of articular cartilage. Changes in the subchondral bone include sclerosis and cystic lesions. Erosive changes, ankylosis, and calcification of the articular cartilage are typically absent.
In the hands, a particular pattern is noted involving the PIP and DIP joints with characteristic sparing of the MCPs (Figure 1A). The first CMC joint is also commonly involved, with bony osteophyte formation and joint space loss. In the knee and hip, loss of joint space with subchondral bone cyst and osteophyte formation is common (Figure 1B).
The cervical and/or lumbar spine may reveal spondylosis, disc space narrowing, and osteophytes. More than 50% of people aged > 65 years have radiologic evidence of OA. However, radiographic evidence of OA is at least twice as common as symptomatic OA, warranting careful consideration when contemplating treatment. 7
Pathogenesis
Normal articular cartilage is a complex tissue composed of extracellular matrix and chondrocytes. Under ideal conditions, hemostasis is maintained with balance between degradation and synthesis of extracellular matrix proteins. In the aging cartilage, a reduction of total proteoglycan synthesis occurs, decreasing its capacity to retain water. Matrix proteins are modified, leading to the accumulation of advanced glycation end products (AGEs). This process is irreversible, and AGEs cannot be removed from the articular cartilage. Chondrocytes respond to AGEs with increased catabolic activity and cytokine release. Initial chondral edema and matrix degradation leads to stress fractures in the collagen network and fissuring of the cartilage. Eventually, the microfractures lead to fragmenting of the cartilage, formation of loose bodies, and synovial inflammation. Sclerosis occurs in the subchondral bone, with accelerated bone turnover leading to osteophyte formation. 8