Dr. Bloor, Dr. Fisher, Dr. Grix, and Dr. Wice are clinical psychologists, and Dr. Zaleon is a clinical pharmacy specialist, all at the VA Ann Arbor Healthcare System in Michigan. Dr. Bloor also is an assistant clinical professor in the psychiatry department at the University of Michigan Medical School in Ann Arbor.
Author disclosures The authors report no actual or potential conflicts of interest with regard to this article.
Disclaimer The opinions expressed herein are those of the authors and do not necessarily reflect those of Federal Practitioner, Frontline Medical Communications Inc., the U.S. Government, or any of its agencies.
With the above concepts in mind, VAAAHS offered veterans conjoint sessions involving a health psychologist and clinical pharmacy specialist during a 3-month period while this resource was available. The conjoint sessions were part of a preexisting pharmacist-run pain medication clinic embedded in primary care. The conjoint session was presented to patients as part of general clinic flow to reduce stigma of engagement in psychological services and allow for the dissemination of BPS information.
Participants
The electronic health records (EHR) of 24 veteran patients with chronic pain, who participated in a conjoint health psychology/pain pharmacy session, were reviewed for the current study. Most of the patients were male (95.8%) and non-Hispanic white (91.7%); the remaining participants did not disclose their ethnicity. The mean age was 60.6 years (SD 7.1; range 50-80). A total of 75% had a mental health diagnosis, and 41.7% were in mental health treatment at the time of the conjoint appointment. Among the sample, 20.8% had a current diagnosis of a substance use disorder (SUD), and no individuals were in treatment for a SUD at the time of the conjoint appointment. Patients received an average of 1.5 conjoint sessions (SD 0.7; range 1-3).
Procedure
The veterans for this project were chosen from a panel of patients followed by the pain medication clinical pharmacy specialist in the primary care pain medication clinic. The selected veterans were offered a joint session with their clinical pharmacy provider and the health psychology resident during their scheduled visit in the pain medication clinic. Each veteran was informed that the goal of the joint visit was to enhance self-directed nonpharmacologic chronic pain management skills as an additional set of tools in the tool kit for particularly difficult pain days. Veterans were assured that their usual care would not be compromised if they declined the session.
During the encounter(s), the health psychologist contributed to the veteran’s care by using MI and CBT for chronic pain skills. The health psychologist further assessed concerns and needs and guided the discussion as appropriate. With veteran readiness, these discussions explored the degree of knowledge and cognitive and behavioral coping skills the patient used. These conjoint sessions also documented the types of discussions and degree of engagement in the encounter(s) as well additional referrals, complementary services, and/or offered follow-up services for either additional conjoint sessions or further health psychology-related services.
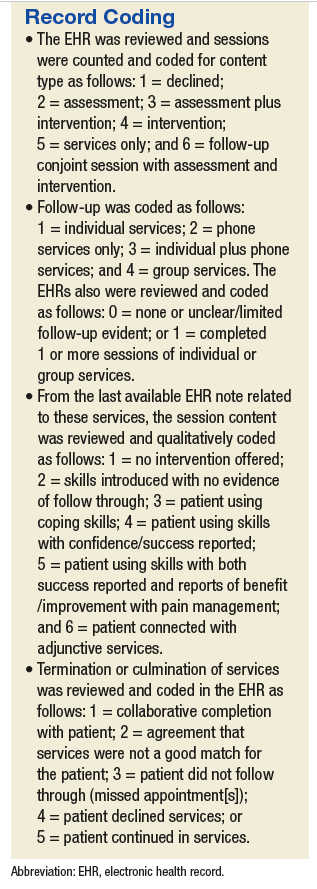
A total of 24 EHRs from these conjoint and subsequent encounters were reviewed for evidence of the procedures by a psychology intern involved in chronic pain management services. Of these 24 records, 6 also were reviewed by a board-certified health psychologist for consensus building and agreement on coding (Sidebar, Record Coding).
Using the coding system and SPSS Version 2.1 (IBM, Armonk NY), descriptive statistics were used to examine conjoint session content and new- or re-engagement in health psychology services following the conjoint sessions. For those patients who followed up with additional services, the content, type, and outcome of these services were explored. Next, linear regression was used to determine whether number of conjoint sessions was associated with a qualitative treatment outcome, and 2 logistic regressions were used to determine whether the number of sessions was associated with the likelihood of accepting services and follow-through with services after accepting them. An additional logistic regression examined whether having a mental health diagnosis (yes/no) was associated with whether the individual accepted additional health psychology services. Finally, independent sample t tests examined differences between those who accepted services vs those who declined follow-up services in substance use diagnosis, mental health diagnosis, and previous health psychology services engagement. Of note, given the small sample size, the Levene’s test for equality of variances was conducted and unequal variances were assumed.
Results
All 24 patients agreed to have the conjoint session with the clinical pharmacy specialist and health psychologist. Of the participants, 62.5% had no previous interaction with health psychology services. Among those who had previous encounters with health psychology services, 12.5% had participated in 1 or more group sessions, another 12.5% had participated in 1 or more individual sessions, and an additional 12.5% had been referred for health psychology services but had not followed through. A total of 10 participants represented a new- or re-engagement in health psychology services following the conjoint appointment. Two patients were referred for additional services as a result of their conjoint appointment (1 to specialty mental health and another to Primary Care-Mental Health Integration [PC-MHI]), and 1 of the participants followed through with the referral. Finally, with regard to the content of the initial session, 37.5% of the sessions contained some form of psychoeducation, 54.2% contained a functional assessment, and 41.7% contained an introduction of skills.