Facilitators
Although the Geriatric SCAN-ECHO program began in January 2013, the VA Greater Los Angeles Healthcare System facility already had several SCAN-ECHO programs. An experienced SCAN-ECHO project director assisted in the implementation of the program. The specialists used existing documents to guide the program, such as a service agreement between SCAN-ECHO and the participating satellite facilities and templates for consults and documentation. Other benefits of the established SCAN-ECHO presence included availability of videoconferencing equipment; local clinical informatics staff who were familiar with the setup of interfacility consults, clinic encounters, and workload credit in the EMR; and PACT clinicians who were familiar with the SCAN-ECHO program and format. Finally, the geriatric interdisciplinary team members had worked together cohesively for years and were supported by the Geriatric Research Education and Clinical Center to implement clinical demonstration projects, such as the SCAN-ECHO program.
Implementation Barriers
Initially the program received few consults. The Geriatric SCAN-ECHO program used a sample case to start the discussion and focused on falls. At times there were also only a small number of facilities and attendees who participated. Most of the attendees were MDs and NPs from Primary Care and Psychiatry. None of the nurses or SWs who were invited by their local leadership participated early on. Informal communication with CBOC staff found that they were feeling overwhelmed with other competing demands. There were multiple SCAN-ECHO programs and no protected time to attend the sessions. In addition, nurses might not have identified the program as a priority because the training topic was too general (geriatrics vs pressure ulcer or pain management).
The Geriatric SCAN-ECHO program adjusted the timing of sessions to convene every other month on a day that most CBOCs had staff meetings, allowing for protected time for staff participation. The CBOC staff was invited again to participate. The gerontological NP contacted the referring clinician to report the date of the case review and followed up afterward to ensure that all questions were answered and recommendations were clear.
The increase in marketing and networking led to more facilities participating; however, the number of staff participants remained low. The program team then changed tactics and focused on facilitating specific clinician behavior changes related to common geriatric syndromes instead of case reviews. The team conducted a session providing an overview of dementia recognition and diagnosis, rationale for objective measures, and a demonstration on the administration of the Mini-Cog Assessment Instrument for Dementia and Montreal Cognitive Assessment (MoCA) tools.7 This session had the highest number of total attendees (38), half of whom were nurses.
Feedback after the session resulted in an additional session the following month, which focused on the scoring and documentation of the tools as well as interpretation of the results and how this might be further evaluated by the team. Informal feedback gathered from nurses during this second session included a request for more training, tips on how to administer the tools, and how to document competency in tool administration. A new educational project that would empower PACT nurses to proactively identify and initiate cognitive impairment/dementia evaluations was then started independent of the Geriatric SCAN-ECHO program.
Results
Participants of SCAN-ECHO programs were surveyed on usefulness of information and its influence on their practice (Table 1). A total of 41 respondents (the same person may have attended more than 1 session) completed surveys on 9 Geriatric SCAN-ECHO sessions. Nineteen (46%) were medical doctors, 8 (20%) were NPs, and 14 (34%) were from other disciplines. Overall, the sessions were well received, and participants found the information useful. Because the respondents were from different disciplines and roles, it was not surprising that only 13 respondents (32%) felt that the information would influence their prescribing practices, and only 18 respondents (44%) agreed that the session changed their ordering of diagnostic tests and studies.
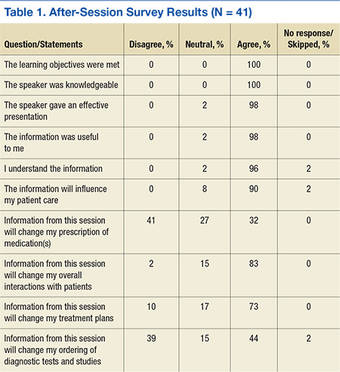
Chart Reviews
Six months after completion of the Geriatric SCAN-ECHO session, the gerontological NP reviewed patient charts and identified rates of adherence for geriatric team recommendations. Eight patient cases were reviewed in 6 of the 9 sessions. The other sessions used sample cases from the team’s experience due to lack of submitted consults. Physicians referred 4 cases, and the rest were from NPs; all were from primary care except for a primary mental health NP. Half of the referred cases were forwarded from other departments (eg, neurobehavior and dementia clinics) to avoid travel. Reasons for referral included geriatric syndrome workup and specific medical questions. All patients were men aged 66 to 94 years (mean = 83.25; SD = 8.29).