Mr. Baker, Ms. Tessier, Ms. Meyer, and Mr. Sones are research assistants in the research department, and Dr. Sachinvala and Dr. Ames are psychiatrists in the psychiatry department, all at the VA Greater Los Angeles Healthcare System in California.
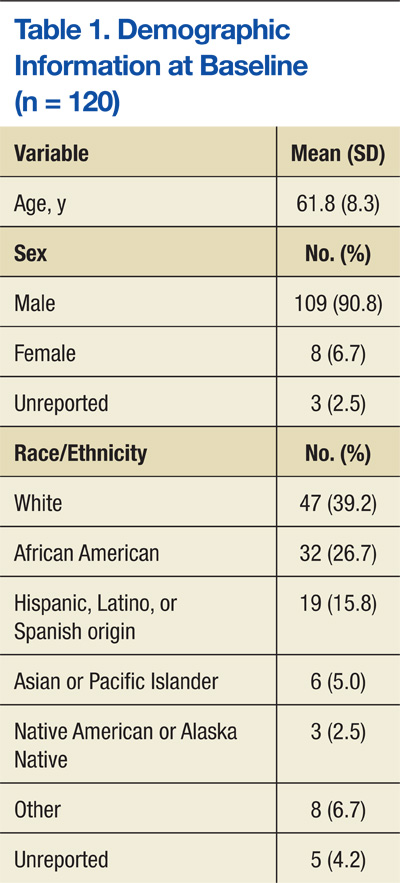
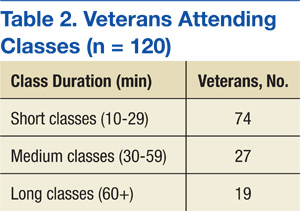
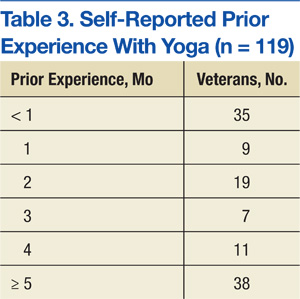
Veterans who completed surveys were predominantly male (90.8%) and averaged 61.4 years of age. Table 1 shows demographic information. Table 2 displays the number of participants who were involved in short (< 30 min), medium (30-59 min), and long (> 60 min) classes. Veteran participants also had a wide range of prior BSR experience (Table 3).
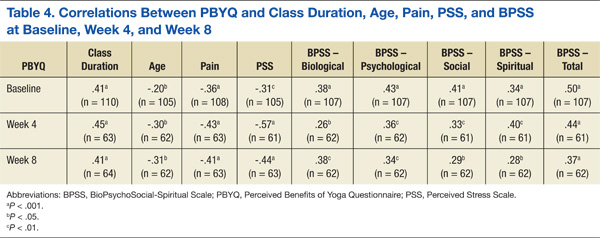
At all time points, PBYQ scores were significantly positively correlated with class duration and biological, psychological, social, spiritual, and total well-being as measured by the BPSS. The PBYQ scores at all time points were also significantly negatively correlated with age, pain ratings, and PSS scores. Table 4 includes specific Pearson’s r values.
Survey week was not significantly associated with any individual outcome measures. There were no significant regressors for total PSS score or total BPSS score within the linear models. However, participants’ PBYQ scores were significantly associated with age (t(98) = -2.13, P = .036), frequency of attendance (t(103) = 2.10, P = .038), and class duration (t(98) = 4.35, P < .001). Additionally, class duration was significantly associated with pain (t(98) = -3.01, P = .003), with longer duration associated with less pain. Ethnicity was also associated with pain, with African American veterans reporting less pain than did white (t(98) = -2.41, P = .017) and Hispanic (t(98) = -2.31, P = .023) veterans. Because ethnicity was significantly associated with class duration (F(5,339) = 3.81, P = .002), the authors used an analysis of covariance to test for a mediating effect of ethnicity on the relationship between class duration and pain. Although there was a partial mediation (F(5,203) = 2.57, P = .028), the main effect of class duration remained significant.
Discussion and Limitations
The goals of this project were to develop a yoga-based program tailored for veterans with SMI and assess the program in a sample of veterans with SMI on subjective reports of stress, pain, well-being, and benefits of yoga. The authors hypothesized that significant improvements in these measures in veterans with SMI would be observed over 8 weeks of participation in BSR classes and that there would be greater benefits in veterans who participated in longer classes and who attended classes more frequently.
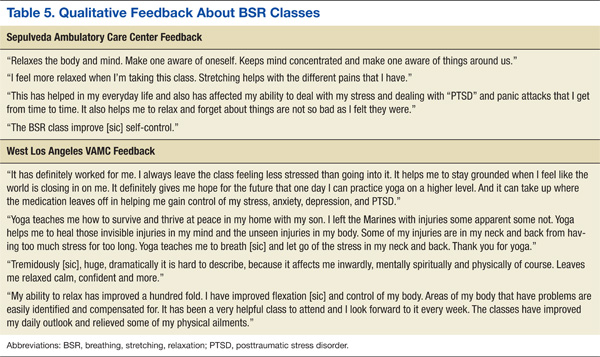
The authors succeeded in developing an adaptable yoga-based wellness program for veterans with SMI that can be both practiced in structured classes and incorporated into veterans’ everyday routines. The BSR classes were well tolerated by veterans with SMI, caused no discernible AEs, and are readily available for dissemination across other mental health programs. Veterans described integrating the tools they learned within BSR classes into their daily lives, helping them to manage pain; feel more flexible; reduce stress, anxiety, depression, and PTSD symptoms; and increase relaxation and feelings of self-control and confidence. Table 5 shows qualitative feedback collected from veterans. In addition, the Train the Trainer model optimized clinical applicability and flexibility, demonstrating that clinicians can seamlessly integrate BSR classes into a health care plan for veterans with SMI.
In assessing quantitative measures of stress, pain, well-being, and perceived benefits of a yoga-based program, veterans who reported BSR classes as beneficial experienced lower levels of pain and stress and higher levels of biological, psychological, social, spiritual, and overall well-being. Those veterans who perceived BSR as more beneficial tended to be younger and attend longer classes with greater frequency. Veterans who attended longer classes also reported experiencing less pain. This may be because the more rigorous stretching and posing involved in longer BSR classes made them more effective at reducing pain; however, it is also possible that veterans who were experiencing more pain avoided these longer classes due to their rigor and length.
Results suggest that longer classes attended with greater regularity may be more beneficial to veterans than short and infrequent classes, particularly in regards to their pain. Despite the relationships between class and outcome variables, the authors did not find significant improvements in measures of wellness, pain, stress, or perceived benefits of BSR over time, as was hypothesized. This may be because the data collection for this study began after classes had been established for some time. In fact, only 35 of 120 veterans included in this study reported having < 1 month of BSR experience at week 0, suggesting that results collected from week 0 did not represent a true baseline measurement. Although no relationship was found between prior duration of attendance and any outcome measures, the fact that most veterans in the sample had attended classes for several months prior to completing surveys may have biased the results by favoring the responses of veterans who were more invested in the classes. Improvements may have been better captured in a BSR-naïve sample.