Hypothermia can also be protective if the victim is breathing when cooling begins, such as while floating or swimming in cold water before drowning.29 This was the likely scenario in a reported case of a Norwegian kayaker who called for help after capsizing in 38°F (3.3°C) seawater. Despite having been in cardiac arrest for over 3 hours, the individual experienced a spontaneous return of circulation and was discharged after 32 days with no neurologic deficits.29
Correcting hypothermia after rescue. Conscious patients with no cardiovascular or respiratory compromise should have wet clothing removed at the scene in exchange for blankets, towels, or warm dry clothing. Advise rescuers to attempt no further rewarming at the scene. With unconscious patients, take only simple measures to prevent further heat loss, and focus on transport and resuscitative efforts.24
Hospital management
Attempts have been made to create a prognostic or predictive scoring system for drowning victims presenting to the emergency department. Factors thought to have bearing on mortality include duration of submersion, victim’s age, Glasgow Coma Scale (GCS) score, pupillary reactivity, and the Acute Physiology and Chronic Health Evaluation II (APACHE II) score.23,30,31 Other measurements, such as core temperature, blood pH, and response to painful stimuli, correlate poorly with mortality.31 Hyperkalemia is repeatedly mentioned as a predictor of a poor neurologic outcome, as it is thought to indicate hypoxia before the onset of cooling.8,26,32 The best predictor of a good outcome is consciousness at the time of arrival at the emergency department.4
Continued ventilation assistance is critical. As with prehospital resuscitation efforts, ventilation is critical to in-hospital management. For patients who are breathing spontaneously, continuous positive airway pressure or bi-level positive airway pressure can reduce hypoxia in pulmonary edema. Standard indications of the need for intubation include decreased level of consciousness or concern for ability to protect the airway, hypoxia despite a high fraction of inspired oxygen (FiO2), or persistent hypercapnia even with adequate noninvasive ventilatory support.33
Victims may swallow large amounts of liquid during drowning; for intubated patients, advise orogastric tube placement to prevent aspiration of gastric contents. The reliability of pulse oximetry has been called into question in this setting and may be less accurate for victims who are hypothermic or who have been submerged in cold water.23,34
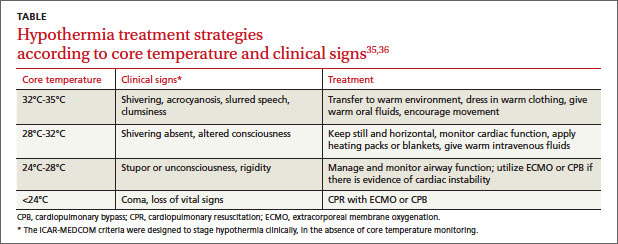
Tiered intervention for hypothermia. In the hospital setting, passive rewarming is indicated for individuals with a body core temperature of 89.6°F to 95°F (32°C-35°C). Remove wet clothing; cover the victim with warm, dry towels or blankets; and give warm oral fluids and urge movement.
Individuals with core temperatures between 82.4°F to 89.6°F (28°C-32°C) require active external rewarming by applying heat directly to the skin via hot packs, warm blankets, and insulation. These patients should remain in a horizontal position with little movement, if possible, to avoid cold peripheral blood rapidly shifting to the core and precipitating an arrhythmia. Warmed intravenous fluids are appropriate as well.
With a core temperature less than 82.4°F (28°C), aggressive rewarming with extracorporeal membrane oxygenation (ECMO) or cardiopulmonary bypass (CPB) may be warranted as this individual will likely have unstable or absent vital signs (TABLE).35,36 Some authorities advise that drowning victims with severe hypothermia and cardiac arrest should be resuscitated at facilities with CPB capability.27,28,37
Inducing hypothermia therapeutically is still unproven. Although not tested specifically on drowning victims, therapeutic hypothermia would seem to have theoretical benefit for their resuscitation. In cardiogenic cardiac arrest, good evidence exists for improved neurologic outcomes with therapeutic hypothermia,38 and this benefit might extend to drowning victims given their similar neurologic injury. No specific pharmacologic therapies have shown benefit in preventing loss of cerebral function.9
Monitor for clinical worsening. The concept of “secondary drowning,” a term now abandoned, referred to the phenomenon of clinical worsening hours after the initial drowning episode and resuscitation. This occurrence is now thought to be due to laryngospasm or to the progressive development of pulmonary edema from the aspiration of small amounts of water. Evidence supports monitoring asymptomatic patients; however, the period of suggested monitoring varies between 4 and 24 hours after the incident.8,22,24
Imaging, if delayed, may be useful. Imaging immediately after a drowning episode is an unreliable predictor of outcome and should be sought only if trauma or symptoms dictate. Cranial computed tomography (CT) has yielded normal findings in drowning victims with a GCS score as low as 4.
If CT is performed, any abnormality detected within 2 to 3 days of injury is a strong predictor of a poor neurologic outcome.39 Magnetic resonance imaging can be beneficial when performed more than 24 hours after resuscitation, preferably within a 4- to 7-day window.20 Lung ultrasound has been used as a bedside tool to monitor progression of pulmonary edema, and could serve the same purpose in drowning recovery.40