Jeremy T. Reed, MD, MPH & TM Colin M. Grant, DO Carl R. Darnall Army Medical Center, Fort Hood, Tex jeremy.t.reed8.mil@mail.mil
DEPARTMENT EDITOR Richard P. Usatine, MD University of Texas Health Science Center at San Antonio
The authors reported no potential conflict of interest relevant to this article.
The opinions and assertions contained herein are the private views of the authors and are not to be construed as official or as reflecting the views of the US Army Medical Department or the US Army at large.
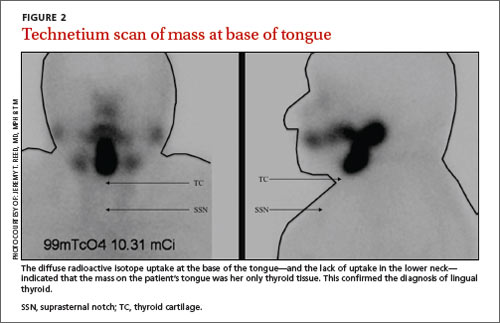
Lingual thyroid results when the thyroid fails to descend from the base of the tongue into the lower neck during early embryongenesis. Based on the clinical presentation and location of the mass, and the fact that it had grown larger during pregnancy, we suspected she had lingual thyroid. This is a rare condition that results from the failure of the thyroid to descend from the base of the tongue into the lower neck during early embryogenesis.1 We ordered thyroid function tests and a technetium scan (FIGURE 2), which showed diffuse radioactive isotope uptake at the base of the tongue and no uptake in the lower neck. This indicated that the mass on the tongue was the patient’s only thyroid tissue and thus confirmed the diagnosis.
The incidence of lingual thyroid is 1 in 100,000.2 Women are affected 4 times as often as men, and approximately 75% of patients have no other thyroid tissue.2 Although the condition often is asymptomatic, patients may present with dysphagia, upper airway obstruction, or hemorrhage. Approximately one-third of patients will present with hypothyroidism.3
Differential diagnosis includes squamous cell carcinoma
The differential diagnosis for a posterior, midline tongue mass is broad. Midline masses are typically congenital and lateral ones are often malignant, inflammatory, or infectious. Tongue lesions include oral squamous cell carcinomas (SCCs), mucoceles, and squamous papillomas.
An SCC of the tongue typically presents as a chronic, nonhealing, irregular mass or ulcer that is hard and bleeds easily with manual palpation. The main causes are constant oral mucosal irritants, usually from smoking, chewing tobacco, or alcohol consumption.4 Firm neck lymphadenopathy is common and signifies local metastasis. Men are affected 2 to 4 times more often than women.5,6 Most patients with SCC are >40 years of age.4
Patients with mucoceles often have a history of oral trauma.7 The rapid appearance of a bluish swelling mass is secondary to salivary gland duct disruption as saliva accumulates in surrounding soft tissues. Mucoceles usually occur in patients <20 years of age and are typically <1 cm in diameter.7 They are most commonly found in the lower lip, yet can occur anywhere in the oral cavity. Most will spontaneously rupture and resolve. Definitive treatment is surgical excision.7
Oral squamous papillomas are the most common benign neoplasms of the oral cavity. They typically appear as solitary pink (nonkeratinized) or white (keratinized) lesions on the ventral surface of the tongue, frenulum, or palate.8 They are common in children and adolescents, but can occur at any age. Most arise spontaneously but they also can be caused by direct contact with infected mucosa.