No lab test to turn to
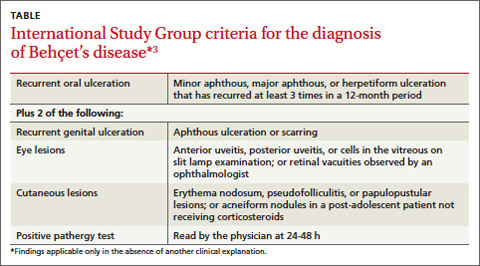
There are no diagnostic laboratory tests for BD; laboratory findings usually reflect systemic inflammation. The International Study Group for BD, however, has derived classification criteria for use in clinical research studies (TABLE).3
Recurrent mouth ulcers—which our patient reported—are essential for the diagnosis of BD. There are typically several such ulcers at any given time and they frequently involve the soft palate and oropharynx. Genital ulceration is the second most common manifestation of BD and is present in 57% to 93% of patients.4 The scrotum is most commonly involved, although the shaft and glans penis may also be affected. Ulcers in the groin and perineum also occur.
Ocular involvement is seen in 30% to 70% of patients and is more frequent and severe in men.5 Panuveitis, posterior uveitis, anterior uveitis, retinal vasculitis, optic neuritis, and retinal vein occlusion cause significant morbidity.
It is induced by a needle prick or injection and is associated with a papule or pustule on an erythematous base. A positive test is defined as a lesion that arises within 24 to 48 hours of the needle prick.