Signs and symptoms
Patients with acute angle-closure glaucoma often develop decreased vision, halos, headaches, severe eye pain, nausea, and vomiting. If the intraocular pressure increases quickly, symptoms can have an acute and dramatic onset; if pressure builds slowly, patients may have limited or no symptoms.4
Physical findings
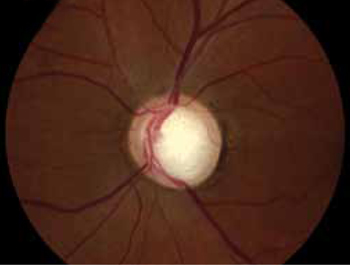
An eye exam will reveal conjunctival erythema, corneal edema and cloudiness, iris irregularity, a shallow anterior chamber (visible with a slit lamp), a dilated pupil (4-6 mm) that reacts sluggishly to light, and increased ocular pressure. The cupping of the optic disc seen in this patient’s retinal exam ( FIGURE 6 ) is more commonly associated with chronic open-angle glaucoma.
FIGURE 6
Management
Acute angle-closure glaucoma is an ophthalmologic emergency, and a referral to a specialist is crucial. If no ophthalmologist can see the patient within an hour of the presentation of symptoms, you’ll need to initiate topical treatment to reduce intraocular pressure and ensure that he or she is seen by a specialist as soon as possible.5 First-line treatments for acute angle-closure glaucoma are listed in TABLE 1 .5,6
In severe cases, topical therapy alone may be ineffective. If there are no contraindications, systemic medications such as acetazolamide, mannitol, glycerol, or isosorbide may be needed. Eye pressure should be checked 30 to 60 minutes after initiating systemic therapy and the patient closely monitored for adverse effects (eg, anaphylaxis, convulsions [acetazolamide]; hypotension [mannitol, isosorbide]).5
When the patient does see an ophthalmologist, the evaluation will include assessment of visual acuity, pupillary evaluation, measurement of intraocular pressure, slit lamp examination, gonioscopy to measure the angle of the anterior chamber, and a fundus exam without pupil dilation.5 Treatment may include a surgical procedure, such as paracentesis of the eye, peripheral iridotomy, or iridectomy, and chronic administration of topical medication.7
TABLE 1
Treatments for acute angle-closure glaucoma5,6
| Medication | Quantity |
|---|---|
| Topical | |
| 0.5% timolol maleate | 1 drop in affected eye 2x/d |
| 1% apraclonidine | 1-2 drops 3x/d |
| 2% pilocarpine | 1 drop 4x/d |
| Oral | |
| Acetazolamide | 500 mg 2x/d |
| Glycerol 50% solution | 1-1.8 g/kg |
| Isosorbide solution | 1.5 g/kg |
| Intravenous | |
| Acetazolamide | 250 mg 4x/d |
| Mannitol | 0.25-2 g/kg (one-time dose) |
CASE 2 The answer is D: Attempt to conduct a visual acuity test and penlight exam without anesthetic; if necessary, apply anesthetic drops and fluorescein stain.
This patient likely has a corneal ulcer or abrasion caused by a contact lens. Corneal ulcers—which constitute a loss of the corneal epithelium—can be caused by trauma or a foreign body, or develop spontaneously.
Signs and symptoms
Because of the rich innervation of the corneal epithelium by the trigeminal nerve, the cornea is highly sensitive to pain. Patients with corneal abrasions typically experience eye pain, photophobia, tearing, a foreign body sensation, and discomfort when driving, working, or reading. If a patient has damage to the trigeminal nerve, however (eg, from trauma, a tumor, or a herpes infection), corneal injuries may be painless.8
In some cases, corneal abrasions may be so painful that patients become disruptive while waiting to be seen. Thus, any patient suspected of having a corneal ulcer or abrasion should be ushered into a quiet, dark room and instructed to keep his or her eyes closed until the examination.
The patient history should focus on recent trauma, type of work, and use of protective eyewear, which may provide clues to the development of penetrating injuries, retained foreign bodies, or abrasions caused by a foreign body. Ask about the use of contact lenses, as well; corneal injury caused by contacts is associated with specific bacterial infections, most commonly staphylococcal organisms and Pseudomonas.9
Physical findings
Attempt to test visual acuity without topical anesthetics. If the patient can’t tolerate the test, a single drop of topical anesthetic (proparacaine 0.5%) may help. Visual acuity provides clues to the location of the injury. If acuity is close to baseline, the corneal abrasion is likely peripheral to the visual axis. Decreased visual acuity indicates either that the abrasion involves the central axis area or that there is corneal edema.9
Evaluation of the pupillary reflex and optic fundus should follow. Reactive miosis may be present with corneal abrasions. A large, nonreactive pupil may be a sign of injury to the pupillary sphincter from blunt or penetrating injury—an ophthalmologic emergency that requires urgent referral. The eyelid should be flipped and examined for foreign bodies. 9
Some abrasions can be seen with the naked eye, so a penlight exam should be performed before applying fluorescein stain. If a corneal lesion is suspicious for herpesvirus infection ( SEE CASE 5 ), fluorescein should not be applied, as it can interfere with the antibody test.10 Refer the patient to an ophthalmologist instead.
If there’s no evidence of infection, apply fluorescein and examine the cornea with a Wood’s lamp. A thin line or several vertical lines are suggestive of a foreign body in the cornea or under the eyelid, whereas round defects are often due to contact lenses.9 Physical findings associated with specific types of corneal abrasions or ulcers are detailed in TABLE 2 .9,11,12