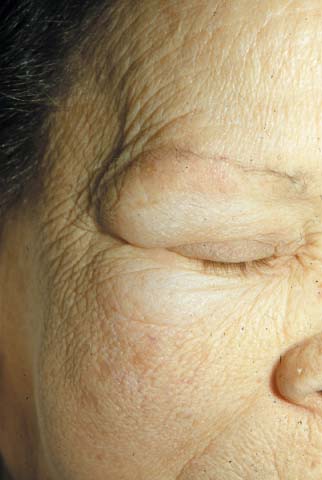
The FP recognized that the patient had hypothyroidism with symptoms of a proximal myopathy. Laboratory testing revealed a highly-elevated thyroid-stimulating hormone (TSH) and a very-low free thyroxine level, confirming hypothyroidism. Her creatinine kinase was also elevated, documenting a proximal myopathy secondary to hypothyroidism. The patient had classic signs of proximal myopathy (she had difficulty climbing stairs, as well as raising her arms over her head to brush her hair), She also had classic signs of hypothyroidism, including skin puffiness, dry and cool skin, hair loss, bradycardia, and a delayed relaxation phase of the deep tendon reflexes. Hypothyroidism does not require an enlarged thyroid gland or goiter as demonstrated by this case.
While the patient needed thyroid replacement, her age and a previous history of ischemic heart disease made it desirable to start levothyroxine at a low dose and titrate up carefully. The FP started the patient on 50 mcg of levothyroxine daily with a plan of increasing the dose by 25 mcg every 2 weeks.
The FP told the patient that if she experienced chest pain on her new medication, she should call the office or go to the emergency department immediately.
The patient responded well to the levothyroxine and didn’t have any cardiac complications from treatment. The patient was followed every 2 weeks with adjustments to her levothyroxine dosing based on symptoms, physical exam, and TSH measurements.
Photo courtesy of the University of Texas Health Sciences Center, Division of Dermatology. Text for Photo Rounds Friday courtesy of Richard P. Usatine, MD. This case was adapted from: Smith M. Goiter and hypothyroidism. In: Usatine R, Smith M, Mayeaux EJ, et al, eds. The Color Atlas of Family Medicine. New York, NY: McGraw-Hill; 2009:954-958.
To learn more about The Color Atlas of Family Medicine, see:
• http://www.amazon.com/Color-Atlas-Family-Medicine/dp/0071474641
You can now get The Color Atlas of Family Medicine as an app for mobile devices including the iPhone, iPad, and all Android devices by clicking this link: