 FIGURE 1 |
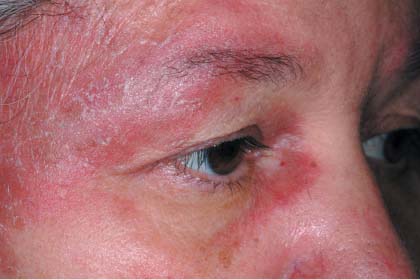 FIGURE 2 |
 FIGURE 3 |
This is a classic presentation of dermatomyositis with the typical rash (FIGURE 1) and proximal muscle weakness. Close attention to the rash around her eyes demonstrates the pathognomonic heliotrope rash of dermatomyositis (FIGURE 2). The heliotrope rash is named after a pink-purple flower, but the rash itself can be more pink than purple.
The patient also had Gottron's papules on the fingers, seen best in this case over the proximal interphalangeal joint of the third finger (FIGURE 3). There was periungual erythema and ragged cuticles, and her scalp was red and scaly. Her neurologic exam was consistent with proximal myopathy. She also had some trouble swallowing bread. (Dysphagia is not unusual in dermatomyositis.) Laboratory tests showed mild elevations in muscle enzymes with the aspartate aminotransferase having the greatest elevation. In other cases, the creatine kinase can be very elevated.
The FP started the patient on 60 mg prednisone daily and topical steroids for the affected areas. The patient responded well to prednisone. Two weeks later, the patient was feeling stronger and the rash was fading. After 6 weeks of 60 mg prednisone daily, she was started on 10 mg methotrexate weekly in order to taper her steroids. The patient continued to do well, but the rash and muscle weakness tended to recur when her steroids were being tapered.
The patient was sent for physical therapy and started on calcium supplementation to protect her from steroid-induced osteoporosis. She was also given 1 mg folic acid a day to minimize the adverse effects of methotrexate.
Since dermatomyositis may be precipitated by an underlying malignancy, the physician screened the patient for internal cancers--especially ovarian cancer. Fortunately, the mammogram, Pap smear, colonoscopy, and abdominal and pelvic CT scans were all normal. Six months later she was doing well on 7.5 mg methotrexate weekly, and 20 mg prednisone daily.
Photos and text for Photo Rounds Friday courtesy of Richard P. Usatine, MD. This case was adapted from: Allred A, Usatine R. Dermatomyositis. In: Usatine R, Smith M, Mayeaux EJ, et al, eds. The Color Atlas of Family Medicine. New York, NY: McGraw-Hill; 2009:772-777.
To learn more about The Color Atlas of Family Medicine, see:
* http://www.amazon.com/Color-Atlas-Family-Medicine/dp/0071474641
The Color Atlas of Family Medicine is also available as an app for mobile devices, see: