Diagnosis: alopecia areata
This is the typical appearance of alopecia areata, a chronic inflammatory disease that affects the hair follicles, causing sudden hair loss. Sometimes it affects the nails as well.1 Alopecia areata occurs in both males and females of all ages and races.
Alopecia areata may be an autoimmune disease, though this is unproven. The affected skin may be slightly erythematous but otherwise appears normal. Short broken hairs (exclamation-mark hairs) may be seen around the margins of expanding patches of baldness. The nails are involved in about 10% of patients with severe enough alopecia to be referred to a specialist.1
Many cases begin in childhood and can be psychologically devastating. Alopecia areata is part of a spectrum of diseases with mild to extensive hair loss (Figure 2), including alopecia totalis, in which all the hair on the scalp is lost, and alopecia universalis (Figure 3), in which all the hair on the body is lost. Extensive involvement, early age of onset, and Down syndrome are all poor prognostic factors for alopecia areata.
FIGURE 2
More extensive alopecia
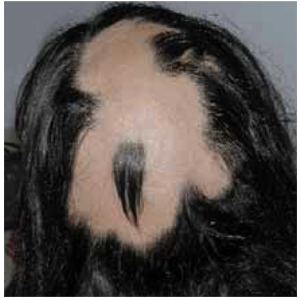
FIGURE 3
Alopecia universalis

Differential diagnoses
The differential diagnosis for alopecia areata includes tinea capitis, trichotillomania, early scarring alopecia, telogen effluvium, anagen effluvium (drug-induced), systemic and discoid lupus erythematosus, and secondary syphilis. In most cases the history and physical exam are adequate to make the diagnosis.
This patient does not have the typical scalp scaling and inflammation seen with tinea capitis. Trichotillomania—hair loss caused by the purposeful pulling of hair by the patient—is likely to cause the most confusion because it coexists with alopecia areata in some cases. This child has shown no evidence of such behavior. She also has no evidence of scalp scarring as may be seen in lupus. Telogen effluvium and anagen effluvium cause a more even distribution of hair loss. The patient has no known risk factors for secondary syphilis.