The follow-up status in 1996 and 1997 of the 104 somatizers and the 66 minor acute illness patients initially rated in 1995 appears in Figure 1. It shows the (percentage) distribution of organic diseases, somatization, and minor acute illness diagnoses for 1995, 1996, and 1997, using all available data in each year. Because our rating of patients in 1 of the 3 categories followed a strict protocol (for 13 patients in 1996 and 40 patients in 1997), and because of insufficient information in their charts, we were unable to definitely ascertain their status. None of the patients with minor acute illness were reclassified as somatizers in the follow-up years, and 83% of these patients continued to have minor acute illness in 1996. All but 2 patients had minor acute illness either in 1996 or 1997 or both. Approximately 27% of the somatizers remained somatizers in 1996, 54% were rated as having minor acute illness, and 13% had organic disease. In 27% of these somatizers minor acute illness developed in the 2 subsequent years. Among patients in 1995, the probabilities of somatization for 2 and 3 consecutive years were 3.7% and 1.1%, respectively. In contrast, for minor acute illness these probabilities were 42.5% and 27%, respectively.
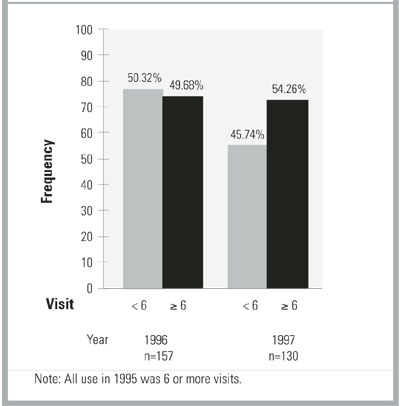
Use status of the groups (somatization, minor acute illness) combined is shown in Figure 2. It shows the (percentage) distribution of use (<6 visits; 6 visits) for 1996 and 1997. Approximately 57% of the somatizers were high users in 1996, compared with 29% of the minor acute illness patients. High use in either 1996 or 1997 was more prevalent among somatizers (70%) than in minor acute illness patients (45%). Persistent high use in both years among minor acute illness patients was 16.7% (95% confidence interval [CI], 8.6%-27.9%) and among somatizers 32.7% (95% CI, 23.8%-42.6%).
TABLE 1
CHARACTERISTICS OF FOLLOW-UP STUDY (N=70)
| Characteristic | Subgroup | Somatizers % (N) | Minor Acute % (N) |
|---|---|---|---|
| Age, years | 20-29 | 13.5 (14) | 9.1 (6) |
| 30-39 | 24.0 (25) | 43.9 (29) | |
| 40-49 | 51.0 (53) | 36.4 (24) | |
| 50+ | 11.5 (12) | 10.6 (7) | |
| Sex | Men | 17.3 (18) | 34.9 (23) |
| Women | 82.7 (86) | 65.2 (43) | |
| Employer | MSU | 6.7 (7) | 4.6 (3) |
| State | 28.9 (30) | 24.2 (16) | |
| GM | 22.1 (23) | 30.3 (20) | |
| Other | 42.3 (44) | 41.0 (27) | |
| Copay, $ | 0 | 58.7 (61) | 57.6 (38) |
| 5 | 28.9 (30) | 25.8 (17) | |
| 7 | 11.5 (12) | 10.6 (7) | |
| 10 | 1.0 (1) | 6.1 (4) | |
| Relationship to subscriber | Self | 59.6 (62) | 62.1 (41) |
| Spouse | 37.5 (39) | 34.9 (23) | |
| Dependent | 2.9 (3) | 3.0 (2) | |
| MSU denotes Michigan State University; GM, General Motors. | |||
FIGURE 1
FOLLOW-UP DIAGNOSES IN INTIALLY IDENTIFIED MINOR ACUTE ILLNESS AND SOMATIZATION PATIENTS
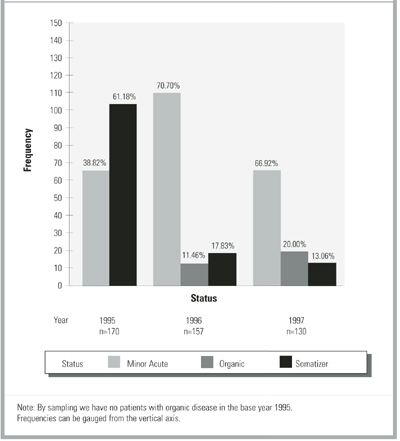
FIGURE 2
FOLLOW-UP USE PATTERNS OF INTIALLY HIGH-USE PATIENTS WITH MINOR ACUTE ILLNESS AND SOMATIZATION PATIENTS
Discussion
Among high users of care, patients with minor acute symptoms were more common than those with symptoms of somatization and organic diseases combined. On follow-up study, diagnoses of somatization often changed to minor acute status, while minor acute illness diagnoses were more persistent. Although use did not remain high in either group, regression to the mean must be considered, because we sampled only on high use in 1995.
We found no research data to compare with our results in patients with minor acute illness. However, the presumed stability and chronicity of somatization diagnoses3,14 have been questioned.14-16 For example, great variability in symptoms was seen in repeated hospitalizations of somatizers, as judged by chart review.17 Others found that only 21 of 70 cases identified as somatization disorder at baseline had the same diagnosis 12 months later and that only approximately one half of all somatization symptoms were present 1 year later.16,18
Limitations
This first preliminary study of high users with minor acute illness was limited by the shortcomings of any retrospective chart review. These include the facts that: (1) We depended on how aggressively a physician attempted to diagnose organic disease and on how completely clinicians recorded their findings; (2) Without access to patients, we were unable to identify their unique perspective or to diagnose specific somatoform disorders3 using, for example, the Diagnostic Interview Schedule,19 the World Health Organization Composite Diagnostic Interview,20 or direct patient interviews; (3) Our designation of somatization depended on identifying symptoms of 6 or more months’ duration, the minimum criterion specified for Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition (DSM-IV) somatoform diagnoses3; if busy clinicians did not record duration, overcoding of minor acute status could have occurred.4 We cannot be certain that patients in either the medically unexplained group (ie, somatization, minor acute illness) did not in fact have organic diseases, because we were unable to investigate each patient ourselves from a biomedical perspective. However, during follow-up chart review, we observed no instances of an important organic disease having been missed when a diagnosis of minor acute illness or somatization status was made initially.15,21
In spite of these expected problems when chart review is the only available source of data, this research on previously unstudied patients provides a starting point for further research. Based on clinical descriptions, our observations on somatizing patients did in fact indicate that we had studied a typical chronic somatizing population (eg, those with low back pain, pelvic pain, irritable bowel syndrome). Also, others have found that chart review may be superior in identifying somatizing patients17,18 and that the DSM-IV has important shortcomings, notwithstanding the latter’s prominent present role in diagnosing conditions with medically unexplained symptoms.22,23 Further, because minor acute illness symptoms are short term, it is arguable that few minor acute patients will receive DSM-IV somatoform diagnoses. Still, as the next research step DSM-IV diagnoses should be sought to better delineate this new group, as should other standard psychiatric measures, especially for depression, anxiety, and unique personality traits.