FIGURE 1
ALGORITHM FOR INITIAL MANAGEMENT OF HYPERTENSION
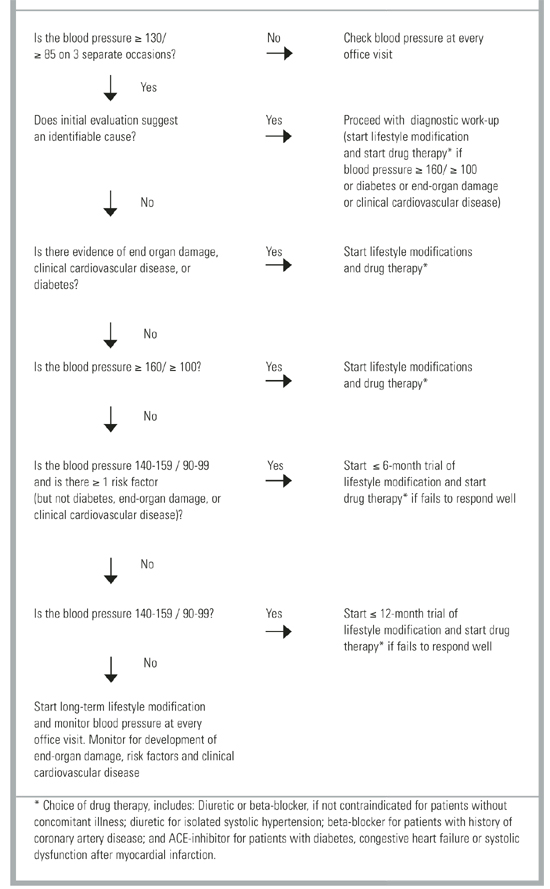
FIGURE 2
ALGORITHM FOR SUBSEQUENT MANAGEMENT OF HYPERTENSION
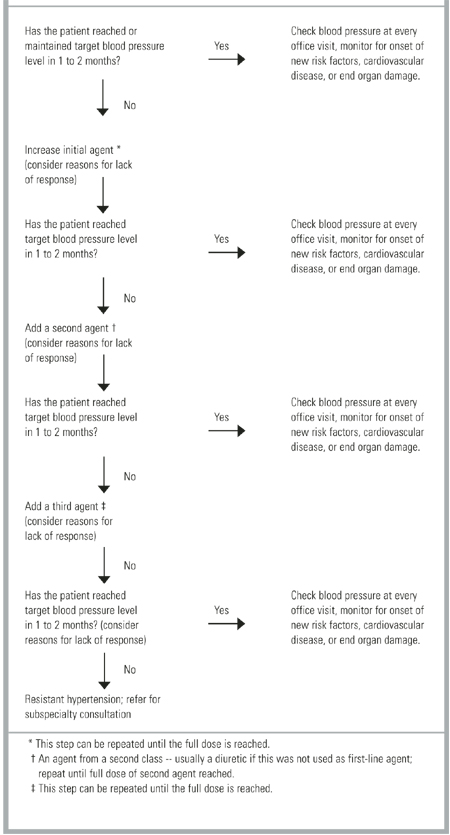
TABLE 2
NUMBER NEEDED TO TREAT (NNT) FOR SPECIFIC ANTIHYPERTENSIVE TREATMENTS
| Medication | Level of Evidence | NNT (95% CI)* | Comment |
|---|---|---|---|
| Low-Dose Thiazide | 1a | 18 (14-23) | Adults with systolic blood pressure |
| ≥ 160 or diastolic blood pressure | |||
| ≥90 regardless of age or comorbidities. | |||
| High-Dose Thiazide | 1a | 67 (48-111) | |
| Beta-Blocker | 1a | 142 (71-1000) | Drug vs no treatment comparison.14 |
| Calcium-Channel Blockers | 1b | 45 (30-102) | Isolated systolic hypertension in older patients, drug vs no treatment comparison.22 |
| ACE inhibitors | 1b | NS | Captopril versus diuretic or ß-blocker. |
| Alpha-agonists | 1b | NS | Doxazosin versus chlorthalidone, increased congestive heart in doxazosin group.7 |
| ARBs | NA | NA | Patient-oriented outcomes not available. |
| Sodium Restriction | 1a | NA | May reduce blood pressure but lacks evidence of reduced morbidity or mortality.27-35 |
| Weight Loss | 1a | NA | |
| Exercise | 1a | NA | |
| Low-Fat Diet | 1b | NA | |
| Limited Alcohol | 5 | NA | |
| Potassium Supplement | 1a | NA | |
| Fish Oil Supplement | 1a | NA | |
| Acupuncture | NA | NA | No evidence of blood pressure reduction or reduced morbidity or mortality.36-43 |
| Biofeedback | NA | NA | |
| Herbal Medicine | NA | NA | |
| Transcendental Meditation | NA | NA | |
| Yoga | NA | NA | |
| *For total cardiovascular events over 5 years. | |||
| NS denotes no significant difference from comparison drug; NA, not applicable; ACE, angiotensin-converting enzyme; ARBs, angiotensin-receptor blockers. | |||
Treatment
Drug Therapy
Patients who require drug treatment for hypertension should begin with a low dose of the initial medication, and that dose should be slowly titrated upward every 1 to 2 months (Figure 2). The JNC-VI recommends a diuretic or a ß-blocker with once daily dosing and 24-hour efficacy as the initial treatment for most hypertensive patients. However, the choice of initial medication will be affected by concomitant illnesses: (1) ß-blockers are recommended for the initial treatment of patients with hypertension and a history of coronary artery disease; (2) diuretics are suggested for the initial treatment of isolated systolic hypertension; (3) and angiotensin-converting enzyme (ACE) inhibitors are recommended for hypertensive patients who have systolic dysfunction after myocardial infarction, diabetic nephropathy, or congestive heart failure. Angiotensin II receptor blockers may be used in patients who cannot tolerate ACE inhibitors because of cough or rash. Alpha-adrenergic blockers should be used with caution in light of evidence that they may increase the risk of cardiovascular events (especially congestive heart failure).7
Among patients who do not have concomitant illness, the choice of drug therapy is controversial. A case-control study and a meta-analysis suggested that short-acting calcium channel blockers (CCBs) increase cardiovascular mortality.8,9 Unfortunately, these studies were not designed to establish a causal relationship. A recent nonsystematic review suggested that short-acting CCBs should be avoided and that conventional therapies were more effective than long-acting CCBs.10 An earlier non-systematic review suggested that short- and intermediate-acting CCBs were associated with increased cardiovascular mortality and morbidity. However, a well-designed cohort study of patients with coronary artery disease failed to reveal an increase in adverse effects among patients taking short-acting CCBs.11 Furthermore, randomized controlled trials suggest that diuretics, ß-blockers, and long-acting CCBs are equally effective in preventing cardiovascular mortality and morbidity.12,13 Physicians who treat hypertension must choose the best initial treatment for patients who do not have concomitant illness. Fortunately, safety, tolerability, efficacy, price, and simplicity can guide the physician to an ideal drug for most hypertensive patients.
Low-dose thiazide diuretics (the equivalent of 25 to 50 mg of hydrochlorothiazide) appear better tolerated than ß-blockers or CCBs.14 Treatment with ß-blockers, CCBs, and ACE inhibitors is also more expensive (75% to 85% more) than diuretic therapy.15 The cost savings offered by diuretics complement the fact that diuretics are safe, effective, and may be dosed once daily. In short, in addition to being the drug of choice for isolated systolic hypertension, low-dose thiazide diuretics are the ideal initial drug treatment of patients without concomitant illness. It should be noted that higher doses of thiazide diuretics offer proportionately less blood pressure reduction and greater risk of hypokalemia.16
Antihypertensive treatment reduces morbidity and mortality for all stages of hypertension, but people with the greatest baseline cardiovascular risk (eg, older patients and patients with higher levels of blood pressure) have the most to gain from treatment.17,18 There is no conclusive evidence to suggest that lowering blood pressure to below 140/80 reduces morbidity or mortality in most patients. However, patients who have diabetes or renal failure benefit from more aggressive management of blood pressure.19,20 Therefore, the JNC-VI recommends a target blood pressure of less than 130/85 for these patients.
The JNC-VI recommendation to start with a low-dose diuretic is supported by the evidence across a spectrum of patient-oriented outcomes. The effectiveness of diuretics and ß-blockers as first-line agents has been confirmed by long-term clinical trials.14,21 However, low-dose thiazides appear effective against a broader range of outcomes than high-dose thiazides and ß-blockers (Table 3). There is also evidence to suggest that CCBs and ACE inhibitors may be effective first-line agents, but fewer patients have been studied who take CCBs and ACE inhibitors than those who take diuretics and ß-blockers.22,23
Most patients with hypertension will respond to 1 (approximately 50%) or 2 (approximately 30%) antihypertensive medications.19,24,25 As noted earlier, failure to respond to treatment suggests an identifiable cause of hypertension. Among patients who do not have a secondary cause of hypertension, inadequate drug treatment (often failure to start a diuretic) and noncompliance are among the most common causes of resistant hypertension.26