Review the need for iron replacement
The role that low levels of iron play in RLS is not entirely clear. One study found the median ferritin level in patients with RLS symptoms to be 33 mcg/L, compared with 59 mcg/L in those without symptoms.18 Another study showed patients with ferritin levels less than 50 mcg/L to have more severe RLS symptoms than those with levels greater than 50 mcg/L.19 Both iron and dopamine have been shown to have circadian rhythms similar to RLS, with their nadir correlating with the time of maximum severity of RLS symptoms. (Low levels of iron may be associated with either idiopathic or secondary RLS.)
Consensus guidelines recommend against initiating iron replacement therapy without checking levels, as this could lead to iron overload.6 Any patient with a plasma ferritin concentration <50 mcg/L and RLS symptoms should be started on iron replacement therapy. The recommended dose of iron is 325 mg ferrous sulfate, taken with 300 mg vitamin C, 3 times a day. Vitamin C allows for better absorption of the iron.8
Monitor ferritin levels at 6-week intervals until they exceed 50 mcg/L, then check iron concentrations every few months. Iron replacement therapy can be decreased or discontinued, provided the ferritin remains at this level.17
Try these strategies for symptom relief
The goal in treating RLS is to decrease the severity and frequency of symptoms, leading to an improvement in sleep quality, a decrease in daytime somnolence, and an overall improvement in quality of life. Treatment guidelines, supported by the IRLSSG and the Medical Advisory Board of the Restless Legs Syndrome Foundation, are based on symptom frequency and severity—whether they are intermittent, daily, or refractory.3,9,17
The algorithm ( FIGURE ) provides recommendations for starting and escalating pharmacologic therapy. Nonpharmacologic treatments have not been studied in systematic trials; however, recommendations for their use are based on expert opinion, case series, or anecdotal reports. In patients who do not have severe symptoms, it makes sense to try simpler strategies first.
Review medications and diet. Many medications have been associated with RLS, either as a secondary cause or suspected of exacerbating symptoms. These include dopamine antagonists (neuroleptics, antiemetics); antidepressants, primarily tricyclics and selective serotonin reuptake inhibitors, lithium, and antipsychotics; antihistamines, including diphenhydramine and other over-the-counter cold and allergy remedies; calcium channel blockers; and diuretics.6,8,17
If a patient troubled by symptoms of RLS is taking any of these agents, consider changing the medication. If no suitable substitute is available, it may help to change the dosing schedule to earlier in the day—ideally no later than 3 PM.8,17 Advise patients, too, to avoid caffeine, tobacco, and alcohol, as well as any other food or beverage known to contain stimulants.
Encourage activity. Discuss the importance of exercise in the management of RLS symptoms. Encourage patients to routinely engage in physical activity and to pursue mentally stimulating activities such as reading, puzzles, or games.
Stress good sleep hygiene. Urge patients to follow a consistent sleep schedule, going to sleep and awakening at the same time each day; to use the bed only for rest or intimacy and avoid reading or watching TV in bed; and to establish a relaxing bedtime routine. Some patients have found that hot or cold baths before bed help to relieve symptoms; others report that massaging their legs or stretching leads to an improvement in symptoms.7,9,17
FIGURE
RLS: A treatment algorithm2,7,9,20
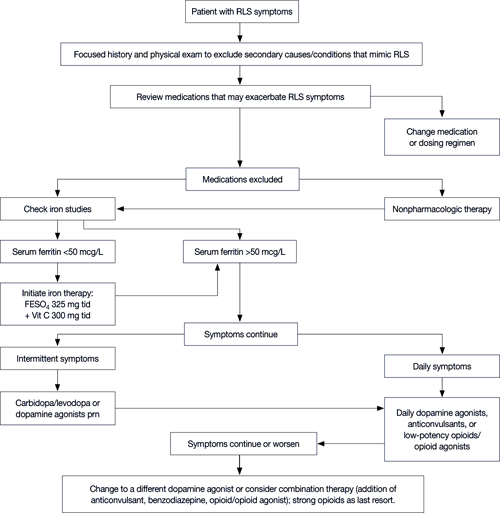
FESO4, ferrous sulfate; RLS, restless legs syndrome.
Pharmacologic options: Selecting the right one
In addition to iron replacement, there are 5 major types of RLS treatment:
- dopaminergic agents,
- dopamine agonists
- anticonvulsants,
- opioids,
- benzodiazepines.
Carbidopa/levodopa for intermittent symptoms
Most patients with RLS have a positive response to treatment with dopaminergic agents, at least initially, and for many years carbidopa/levodopa was the usual therapy for RLS. It remains a first-line treatment for patients with intermittent symptoms.
Early studies consistently showed that 70% to 80% of RLS patients treated with carbidopa/levodopa had a significant improvement in symptoms.20-22 But the studies were small, did not always include a placebo arm, and most were crossover trials, making it impossible to do a statistical comparison.5