There is general agreement about the need to exclude other potential etiologies of lower urinary tract symptoms in older men.4,15 Thus, you need to consider such causes as urinary tract stones, infections, or cancer; comorbid conditions that may affect bladder function or lead to polyuria; drug side effects; or sleep disturbances associated with chronic insomnia, depression, ethanol abuse, or sleep apnea.13,14
FAST TRACK
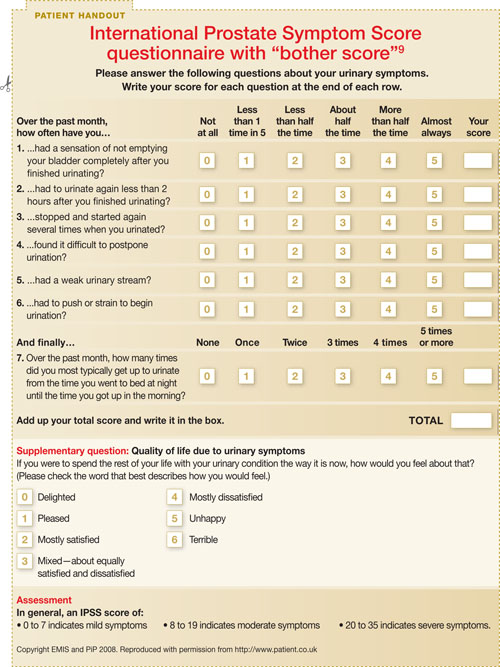
The quality-of-life question is a good indicator of whether watchful waiting is preferred over active treatment
Digital rectal exam (DRE). The physical exam should include both a DRE and a search for neurological deficits to look for evidence that lower urinary tract symptoms are not BPH-related. The DRE should assess for stool impaction and prostate symmetry, nodularity, and consistency. Prostate volume estimates by DRE are not reliable and generally underestimate actual values while correlating poorly with BPH symptoms.14,18
Urinalysis. If you suspect BPH, you'll need to order a urinalysis to screen for infection, cancer, or stones and additional lab studies based on the patient's history, including measurements of serum creatinine, calcium, glucose, and prostate-specific antigen (PSA), among others.4,15
PSA values. These values should be checked if the patient's life expectancy is greater than a decade and a diagnosis of prostate cancer would influence treatment decisions. Adjustments of accepted norms should account for increasing age (40 to 50 years, 0-2.5 ng/mL; 51 to 60 years, 2.5-3.5 ng/mL; 61 to 70 years, 3.5-4.5 ng/mL; 71 to 80 years, 4.5-6.5 ng/mL), and urologic referral should be made as indicated.18
PSA determination is a more accurate reflection of prostate volume than a DRE and helps establish a pretreatment reference point before 5-a reductase inhibitor therapy.19 These drugs lower PSA concentrations approximately 50% and may complicate subsequent cancer screening.15
The US Preventive Services Task Force (USPSTF) clinical guidelines for prostate cancer screening notes that among patients with enlarged prostates, the specificity of PSA testing is lower, and thus PSA is a less accurate means of detecting cancer in BPH patients.20 Indeed, the USPSTF guidelines are ambivalent on the utility of PSA, in part because of the heterogeneity of prostate tumors, although they do confirm the greater accuracy of PSA testing over DRE.20
The guidelines state that screening is most effective at determining patients with a particularly good or poor long-term prognosis, which constitutes a fairly small minority of patients, but is less effective in the larger middle group.20 Regarding the particular means of testing PSA, the USPSTF guidelines note that free or complex testing is primarily useful to distinguish whether a patient should undergo a biopsy among those with a PSA level of 4.0 to 9.9 ng/mL.20 A more recent perspective from Cleveland Clinic clinicians indicates that the "PSA cutoff era" is now past and that decisions for further prostate cancer screening should be made with a patient's DRE and family history data in mind.21
Diagnostic studies. Noninvasive urine flow rates, postvoid residual measures, pressure-flow studies, cystoscopy, and renal or transrectal ultrasound are optional unless dictated by specific circumstances, including recurrent hematuria, pelvic pain, or urinary retention, in which case urologic consultation is indicated.4,15
FAST TRACK
PSA is a less accurate means of detecting cancer in BPH patients
Weigh patient preference against symptom severity
The treatment goals for a patient with BPH-related lower urinary tract symptoms must focus on improving and maintaining quality of life, achieving and sustaining symptom control, and avoiding disease progression.22 In choosing a specific treatment, weigh the patient's preferences against symptom severity and specific physiologic variables; even individuals with moderate IPSS ratings may improve (40%) or show no change (45%) with watchful waiting.23 (The AUA outlines treatment options for patients with moderate to severe symptoms in its BPH practice guidelines. They can be accessed on page 16 of http://www.auanet.org/guidelines/main_reports/bph_management/chapt_1_appendix.pdf.
Quality-of-life issues—how much lower urinary tract symptoms interfere with work, social life, sleep, sexual function, and travel—are generally more important than the symptoms per se.14 The AUA has published a diagnosis and treatment algorithm for BPH that is very helpful for practitioners.4 It is available on page 7 of http://www.auanet.org/guidelines/main_reports/bph_management/chapt_1_appendix.pdf.
Watchful waiting—even with high IPSS ratings
Watchful waiting is an option for patients experiencing minimal bother—even with high IPSS ratings—because the risk for progression is relatively small.4,14,15 If you choose this route, encourage the patient to minimize alcohol and caffeine use and the intake of fluids in the evening, and minimize the use of a-agonist, anticholinergic, antihistaminic, and calcium-channel blocker medications.