The patient’s signs and symptoms:
- Skin folds on the neck
- Decreasing visual acuity
- Skin biopsy showing irregular aggregates of clumped, thickened, elastic fibers in the papillary and reticular dermis
A 21-year-old woman came to the British American Hospital in Lima, Peru, complaining of skin folds that had been growing on her neck for 3 years, as well as decreasing visual acuity over the last several months. She said that the skin folds were neither itchy nor painful.
She had a history of heartburn that worsened after eating, but that was being treated successfully with ranitidine. She reported no fever, chills, sweats, weight loss, alopecia, photosensitivity, malar rash, or any other skin rashes. Her history was otherwise unremarkable. She was taking no medications other than ranitidine, and had no known drug allergies. She didn’t smoke and drank alcohol only occasionally. Our patient worked as a salesperson at a music store. Interestingly, she had a sister with the same skin lesions and ophthalmologic complaint.
We found no lymphadenopathy. On her antecubital fossae and neck, numerous small, yellow papules had coalesced to form plaques with a cobblestone appearance (FIGURE 1). Her skin was redundant in the neck and axillae. We noted no other skin folds. She had a prominent horizontal crease of the chin (positive mental crease sign).
There were angioid streaks on funduscopic examination (FIGURE 2). Her lungs were clear to auscultation and percussion. Her cardiovascular exam was normal; there were no carotid bruits, and peripheral pulses were normal. The abdomen was soft and nontender; no hepatosplenomegaly or masses were present. We found no peripheral edema or cyanosis. A neurological exam was unremarkable.
Blood work revealed a hemoglobin level of 11.8 g/dL. The rest of the complete blood count was within normal limits. Electrolytes, liver profile, lipid profile, and urinalysis were within normal limits. A chest film showed no acute process. Skin biopsy of the neck folds showed irregular aggregates of clumped, thickened, elasticfibers in the papillary and reticular dermis (FIGURE 3).
FIGURE 1
Skin folds that had been growing for 3 years

In addition to the skin folds on her neck, the patient had several small, yellow papules that had coalesced to form plaques with a cobblestone appearance.
FIGURE 2
Cause of the patient’s declining vision

A funduscopic exam revealed angioid streaks (arrows).
FIGURE 3
Skin biopsy results
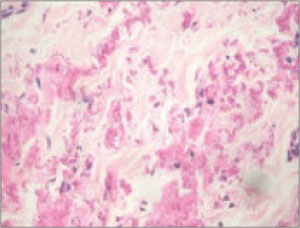
Biopsy of the patient’s skin folds showed irregular aggregates of clumped, thickened, elastic fibers in the papillary and reticular dermis. No epidermal changes were appreciated (hematoxylin and eosin stain).
What is your diagnosis?
Diagnosis: Pseudoxanthoma elasticum
Pseudoxanthoma elasticum is an autosomally inherited disorder associated with the accumulation of mineralized and fragmented elastic fibers in the skin, Bruch’s membrane in the retina, and vessel walls.1,2 The patient’s dermatologic and ocular findings were highly suggestive of this disorder, particularly given the absence of findings indicative of other diseases.
The average age of patients diagnosed with pseudoxanthoma elasticum skin abnormalities is 22 years.3 Risk of cardiovascular disease may correlate with the presence of angioid streaks of the fundus—irregular, reddish-brown, or gray lines radiating from the optic disc.4 Patients may have severe ophthalmologic or cardiac disease with little or no skin involvement, or vice versa.5-8 Onset, progression, and severity of the disease vary considerably among patients.8,9
With timely diagnosis, many complications of pseudoxanthoma elasticum can be prevented or treated. In particular, prognosis improves with early recognition of extracutaneous organ involvement. Screen first-degree family members for any cutaneous or ophthalmologic markers of pseudoxanthoma elasticum, and offer genetic counseling to family members of affected patients.
Estimated prevalence ranges from 1:70,000 to 1:100,000 live births,10 which may vary in specific areas. In 2000, the patient support group PXE International suggested that there is a prevalence of 1:25,000 in New England.11 The female-to-male ratio is thought to be almost 2:1, but there is no satisfactory explanation for this. All races are affected.
Clues to look for in the 3 systems affected
Dermatologic manifestations. The most common features of pseudoxanthoma elasticum are ivory to yellowish, raised papules varying in size from 1 to 3 mm. The papules may have a linear or reticular arrangement and may coalesce into plaques.12 In many patients the skin becomes wrinkled and redundant, hanging in folds, as was the case with our patient. The lesions occur first on the lateral part of the neck and the flexural areas.
Isolated periumbilical skin lesions are called periumbilical perforating pseudoxanthoma elasticum, but there is no known relation with hereditary pseudoxanthoma elasticum.13 The mental crease sign is considered a sign of pseudoxanthoma elasticum.14 The scalp, palms, and soles are unaffected. Lesions on the mucous membranes are common, especially on the inner aspect of the lower lip.