Diagnosis: Misplaced eyelash
The life cycle of eyelashes is usually an asymptomatic process. Sometimes, though, lashes can find their way into unusual anatomical sites, as occurred in the 5 cases described on the previous page. Here, broken down by the location in which the eyelash was found, is a discussion of the trouble a misplaced eyelash can cause.
Punctum: Upper is more common than lower
Once an eyelash is shed into the external ocular surface, it can cause foreign body sensation, leading to reflex tearing that will carry it away to the lacus lacrimalis. At this point, it comes in close contact with the punctum and can be propelled by the lids or sucked into the canaliculus in the blink cycle.
If it finds its way into the punctum, the barbs on the hair prevent it from being expelled. They can obstruct the canaliculi, causing epiphora, or incite inflammation and possibly infection, causing canaliculitis or dacryocystitis.1
Eyelashes are often reported to enter the upper and lower punctum, though Nagashima and Kido found that cilia in upper punctum was 3 times more frequent than cilia in the lower punctum.2
In CASE 1, involving mild erythema of the nasal bulbar conjunctiva and linear corneal abrasions, the 35-year-old patient had an eyelash protruding from the upper punctum. The rest of the exam was unremarkable. His physician removed the eyelash mechanically, without resistance. This relieved his symptoms and he was given a prophylactic topical antibiotic.
In CASE 2, the 23-year old woman with bulbar conjunctival injection and linear corneal abrasions, there was an eyelash projecting out of the lower punctum. The eyelash was removed easily and she, too, was treated with topical antibiotic ointment.
CASE 1 Upper punctum
Eyelash protruding from the upper punctum.
CASE 2 Lower punctum

Meibomian gland: An uncommon spot
Cilia in the meibomian gland is unusual. Clinicians who suspect this is the cause of a patient’s discomfort will need to differentiate it from acquired distichiasis, which is metaplastic eyelash growth that results from chronic lid inflammation. Careful examination, and the absence of resistance on removal, differentiate the 2 conditions.
In CASE 3, involving the 28-year-old man with eye irritation and photosensitivity, an examination showed an eyelash protruding from a meibomian gland orifice 2 mm lateral to the lower punctum. He also had corneal punctate epithelial erosions and mild ciliary flush. His physician removed the eyelash with forceps without resistance. He was given a topical antibiotic.
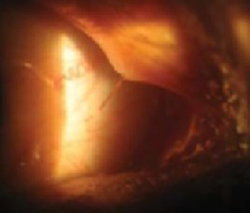
In CASE 4, involving the 15-year-old pictured on page 365 who had been unsuccessfully treated with different lubricants and antibiotics for exposure keratopathy, an examination revealed shortening of the upper and lower eyelids of the affected eye and abnormal upper eye lid contour causing 4 to 5 mm of lagophthalmos. She had a positive Bell’s phenomenon and normal tear break-up time.
Further examination of the upper eyelid margin, pictured at far right, showed a cilium projecting out of a meibomian gland orifice toward the ocular surface with corneal punctuate erosions. The eyelash was removed smoothly with forceps without resistance, and her symptoms resolved within a few days.