Practice recommendations
- Obvious anxiety in a patient with physical complaints should prompt an evaluation for somatization.
- Become familiar with the 4 patterns of somatization and their manifestations.
- Learn how to conduct an emotion-focused interview, which, when applied appropriately, will help rule somatization in or out.
A 42-year-old man has chronic fatigue and fibromyalgia that has led to a 13-month disability leave from work. The reason for his current office visit is longstanding pain in his shoulders. As you take his history, he is sitting with hands clenched and he generally appears tense.
A 38-year-old woman with severe incapacitating gastroesophageal reflux disease, irritable bowel syndrome, and depression has been too disabled to work for 2 years. At the time of your interview, her posture is relaxed and she shows no signs of anxiety.
These 2 very different patients (whose cases I will review in detail) share a common problem: somatization, the translation of emotions into somatic problems or complaints. It is well documented—though still largely unrecognized in practice—that somatization accounts for a large proportion of office visits to primary care physicians as well as specialists,1,2 leading to unnecessary testing, treatment, and hospitalization, disability and corporate financial loss,3 likely earlier mortality,4 and frustration for patients and physicians.5
No longer a diagnosis of exclusion
Despite the burden somatization places on the medical system, the diagnosis is often made by indirect methods such as checklist, speculation, or exclusion when other problems are ruled out.6 The common position, even in recent reviews, is that somatization should be treated by nonspecific measures, such as frequent office visits to increase the patient’s and physician’s ability to cope with what is often seen to be a chronic and incurable disorder.7-11 Such a position is no longer warranted.
Based on recent quantitative and extensive case-based research, specific emotion-focused brief therapies and videotape-based research have clarified how emotions are experienced in the body and how somatization of emotions occurs (see The physiology of emotions). These methods, including short-term dynamic psychotherapy (STDP) have been used to diagnose and treat somatization effectively since the 1980s. Somatization, with its morbidity and chronicity, need no longer be diagnosed by exclusion nor treated palliatively without specific diagnostic testing.
The physiology of emotions
To diagnose and manage somatization we must know how emotions are experienced and how they may become somatized. Davanloo discovered through studying several hundred case videotapes that specific emotions manifest in specific ways regardless of gender, age, or ethnicity.12 This emotion physiology constitutes a norm to compare with a patient who somatizes emotions.
For example, rage is experienced as an internal energy sensation, heat, or “volcano” that rises from the lower abdomen to the chest, neck, and finally to the hands with an urge to grab and do some form of violence. Guilt about rage is experienced with upper chest constriction or even pain, intense painful feeling with waves of tears and with thoughts of remorse about experiencing the rage.13 When feelings are experienced consciously, by definition they are not being somatized at that moment.
Why somatization occurs
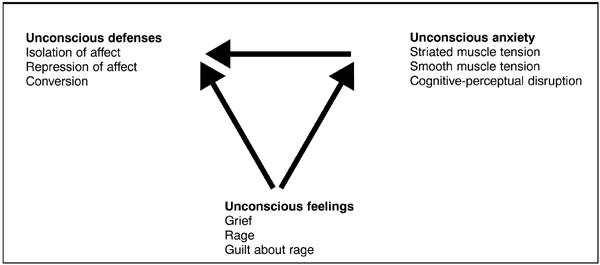
When feelings are intense, frightening, or conflicted, they create anxiety and defense mechanisms to cover the anxiety (see the Figure ). If these feelings are unconscious to the patient, the subsequent anxiety and defenses may also be outside of awareness.
This is the finding common in people who have been traumatized by someone close to them: feelings of rage toward a loved one are unacceptable, frightening, and avoided through somatization and other defenses.14 Diverse research has found that patients with hypertension, migraine, irritable bowel syndrome, and other conditions internalize anger and thus increase their somatic problems.15-17 Blocking and inhibiting of emotions, including anger, is a common finding in somatizing patients.
FIGURE
The 4 patterns of somatization
Videotaped case-series research shows 4 main patterns of somatization: 1) striated muscle unconscious anxiety, 2) smooth muscle tension 3) cognitive-perceptual disruption, and 4) conversion.18
Striated muscle tension due to unconscious anxiety manifests through hand clenching, sighing, and even hyperventilation that the patient is not aware of. These patients may report panic attacks, chest pain, headache, fibromyalgia, and other musculoskeletal complaints. These conditions are often frustrating to family, employers, and physicians since conditions like chronic pain respond to treatment slowly or not at all.
Smooth muscle tension due to unconscious anxiety causes acute or chronic spasm of blood vessels, GI tract, airways, and the bladder. Patients exhibiting smooth muscle tension may present with GI symptoms, migraine, hypertension, urinary frequency, and upper airway constriction mimicking asthma. They often report histories of depression, panic, substance abuse, personality disorders, and past sexual or physical abuse.