It is essential that patients receive counseling and give informed consent regarding the risks and benefits of observation or induction for isolated term oligohydramnios. The ease of induction based on parity and cervical ripeness should be considered.
A primiparous woman with an unfavorable cervix who strongly desires a spontaneous, vaginal birth could be told that, although there may be a small risk for her baby, no study has demonstrated any increased long-term morbidity or mortality associated with low fluid in her situation and that labor induction may double her chance of cesarean delivery.37,38 In such a situation, an acceptable approach for mother and clinician may be rehydration followed by a repeat AFI and close follow-up with testing for fetal well-being according to the algorithm (Figure). In a practical sense, rehydration with 2 liters of oral water for oligohydramnios may be done whether or not immediate induction is chosen, as this is a safe measure that has been shown to significantly increase AFI. Alternatively, the preferred approach for a multiparous woman with a ripe cervix by Bishop score may be labor induction.
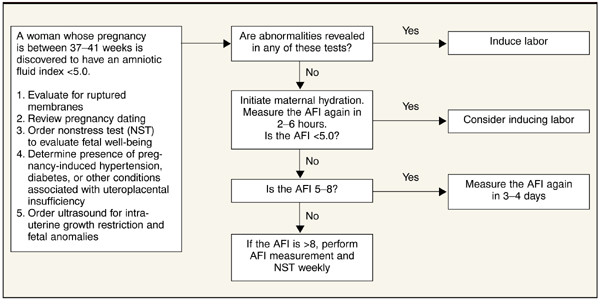
As adverse fetal outcomes have not been demonstrated in women with isolated term oligohydramnios, there is no rationale for routinely inducing labor based on an isolated finding of a so called “borderline” amniotic fluid index in the 5-to-8 range. In this situation it is appropriate to perform the initial assessment described above and may be reasonable to repeat the amniotic fluid index in 3 to 4 days to determine if true oligohydramnios has developed.
FIGURE Assessment of the pregnant woman with oligohydramnios at term
Acknowledgments
We appreciate the assistance of George Gilson MD, Lauren Plante MD, and William Rayburn MD in manuscript review.
Corresponding author Lawrence Leeman, MD, MPH, University of New Mexico Depts of Family and Community Medicine, Obstetrics and Gynecology, 2400 Tucker NE, 3rd floor, Albuquerque, NM 87131. E-mail: lleeman@salud.unm.edu.